Mastoid Obliteration with Silicone Blocks after Canal Wall Down Mastoidectomy
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Chonnam National University Medical School, Gwangju, Korea. victocho@hanmail.net
Abstract
OBJECTIVES
To evaluate the usefulness of silicone blocks as graft material for mastoid cavity obliteration in the prevention of problematic mastoid cavities after canal wall down mastoidectomies.
METHODS
Retrospective evaluation of 20 patients who underwent mastoid obliteration with silicone blocks between 2002 and 2009 at the Chonnam National University Hospital. The cases consisted of 17 patients with chronic otitis media with cholesteatoma and 3 patients with adhesive otitis media. The postoperative follow-up period was an average 49 months (range, 6 to 90 months). The surgical technique used at our institution composed four major steps: First, the canal wall down mastoidectomy was performed and the middle ear procedure was completed. The silicone blocks were used to fill up the mastoidectomized cavity. Then, a cortical bone pate was used to cover the surface of the silicone blocks. Finally, temporalis fascia and a split musculoperiosteal flap were used to surround the bone pate for reinforcement of the reconstructed canal wall. We examined postoperative success rate and hearing outcomes.
RESULTS
In 19 cases (95%), the reconstructed canal wall maintained a cylindrical shape and the ear drum healed without perforation. In only 1 case (5%), the reconstructed canal wall was destroyed with ear drum perforation. The mean improvement in air-bone gap was about 12 dB (P<0.05), and the mean improvement in air-conduction was about 16 dB (P<0.05).
CONCLUSION
We suggest that silicone blocks could be valuable resources as graft materials for mastoid obliteration after canal wall down mastoidectomies.
MeSH Terms
Figure
-
Fig. 1 Silicone (Hansbiomed Co., Daejeon, Korea) is soft enough to be cut by scarpel and easy to be designed, but solid enough to exist in the mastoid lifelong.
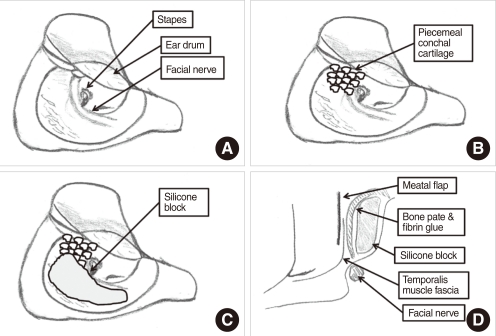
Fig. 2 Schematic figures of operating technique. (A) A canal wall down mastoidectomy is performed for removing of diseases. (B) The epitympanic cavity is obliterated with piecemeal cartilage. (C) Mastoid cavity is obliterated with silicone blocks. (D) Coronal view. Silicone blocks are covered with bone pate and temporalis muscle fascia.
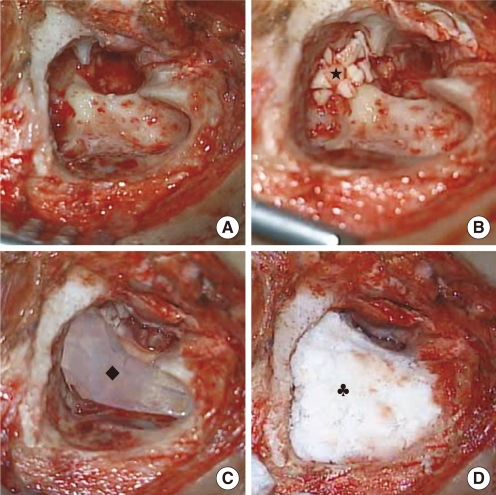
Fig. 3 Surgical procedures for mastoid obliteration with silicone blocks and bone pate. (A) After elevation of the anterior-based flap, a canal wall down mastoidectomy is performed. (B) The epitympanic cavity is obliterated with piecemeal cartilage. (C) Silicone blocks are used to fill the mastoid cavity. (D) Silicone blocks are fixed using fibrin glue and covered with bone pate. ★, piecemeal conchal cartilage; ◆, silicone block; ♣, bone pate.
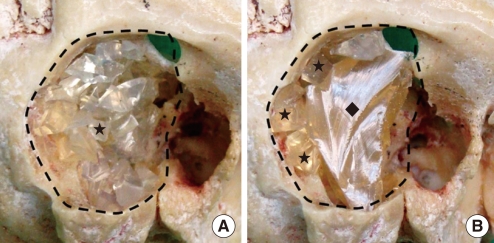
Fig. 4 Group A, mastoid obliteration with piecemeal silicone blocks and filling with bone pate. Group B, mastoid obliteration with large silicone block and supplying the deficiency with piecemeal silicone blocks and bone pate. Dotted line, mastoid cavity; ★, piecemeal silicone blocks; ◆, large silicone block.
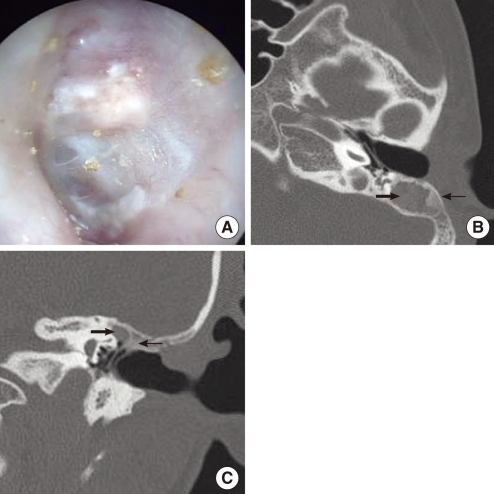
Fig. 5 Postoperative findings after mastoid obliteration (7 months after surgery). (A) Photograph of drum and external auditory canal. Reconstructed posterior wall is well maintained. (B, C) Axial and coronal temporal bone CT scan. The mastoid cavity is well obliterated by the silicone blocks (thick arrow) and bone pate (thin arrow).
Reference
-
1. Palva T. Operative technique in mastoid obliteration. Acta Otolaryngol. 1973; 4. 75(4):289–290. PMID: 4702622.
Article2. Sade J, Weinberg J, Berco E, Brown M, Halevy A. The marsupialized (radical) mastoid. J Laryngol Otol. 1982; 10. 96(10):869–875. PMID: 7119556.3. Shelton C, Sheehy JL. Tympanoplasty: review of 400 staged cases. Laryngoscope. 1990; 7. 100(7):679–681. PMID: 2362526.4. Whittemore KR Jr, Merchant SN, Rosowski JJ. Acoustic mechanisms: canal wall-up versus canal wall-down mastoidectomy. Otolaryngol Head Neck Surg. 1998; 6. 118(6):751–761. PMID: 9627232.5. Gantz BJ, Wilkinson EP, Hansen MR. Canal wall reconstruction tympanomastoidectomy with mastoid obliteration. Laryngoscope. 2005; 10. 115(10):1734–1740. PMID: 16222186.
Article6. Shea MC Jr, Gardner G Jr, Simpson ME. Mastoid obliteration using homogenous bone chips and autogenous bone paste. Trans Am Acad Ophthalmol Otolaryngol. 1972; Jan-Feb. 76(1):160–172. PMID: 4337026.7. Black B. Mastoidectomy elimination: obliterate, reconstruct, or ablate? Am J Otol. 1998; 9. 19(5):551–557. PMID: 9752959.8. Dornhoffer JL. Surgical modification of the difficult mastoid cavity. Otolaryngol Head Neck Surg. 1999; 3. 120(3):361–367. PMID: 10064639.
Article9. Grote JJ. Results of cavity reconstruction with hydroxyapatite implants after 15 years. Am J Otol. 1998; 9. 19(5):565–568. PMID: 9752961.10. Ringenberg JC, Fornatto EJ. The fat graft in middle ear surgery. Arch Otolaryngol. 1962; 11. 76:407–413. PMID: 13973971.
Article11. Moffat DA, Gray RF, Irving RM. Mastoid obliteration using bone pate. Clin Otolaryngol Allied Sci. 1994; 4. 19(2):149–157. PMID: 8026095.12. East CA, Brough MD, Grant HR. Mastoid obliteration with the temporoparietal fascia flap. J Laryngol Otol. 1991; 6. 105(6):417–420. PMID: 2072006.
Article13. Cheney ML, Megerian CA, Brown MT, McKenna MJ. Mastoid obliteration and lining using the temporoparietal fascial flap. Laryngoscope. 1995; 9. 105(9 Pt 1):1010–1013. PMID: 7666712.
Article14. Mahendran S, Yung MW. Mastoid obliteration with hydroxyapatite cement: the Ipswich experience. Otol Neurotol. 2004; 1. 25(1):19–21. PMID: 14724486.
Article15. Kakigi A, Taguchi D, Takeda T. Mastoid obliteration using calcium phosphate bone paste with an artificial dermis soaked with basic fibroblast growth factor: preliminary clinical report. Auris Nasus Larynx. 2009; 2. 36(1):15–19. PMID: 18485642.
Article16. Ridenour JS, Poe DS, Roberson DW. Complications with hydroxyapatite cement in mastoid cavity obliteration. Otolaryngol Head Neck Surg. 2008; 11. 139(5):641–645. PMID: 18984257.
Article17. Bondurant S, Ernster VL, Herdman R. Institute of Medicine, Committee on the Safety of Silicone Breast Implants. Safety of silicone breast implants. 2000. Washington, DC: Institute of Medicine.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Modified Canal Wall Down Mastoidectomy Without Meatoplasty
- Outcomes of Modified Canal Wall Down Mastoidectomy and Mastoid Obliteration Using Autologous Materials
- Partial Mastoid Obliteration Using Inferior Based Musculoperiosteal Flap and Autogenous Conchal Cartilage Chips
- Reconstruction of the Posterior Canal Wall with Mastoid Obliteration after Canal Wall Down Mastoidectomy
- A Case of Repair of Retroauricular Skin Defect and Mastoid Cavity with Posterior Wall Reconstruction Using Tutoplast(R)(Allograft Cancellous Bone Chip) and Bone Dust after Canal Wall Down Mastoidectomy
