Clin Exp Otorhinolaryngol.
2014 Dec;7(4):264-268. 10.3342/ceo.2014.7.4.264.
Hearing and Facial Function After Surgical Removal of Cholesteatomas Involving Petrous Bone
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jwchung@amc.seoul.kr
- 2Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. yscho@skku.edu
- KMID: 2278365
- DOI: http://doi.org/10.3342/ceo.2014.7.4.264
Abstract
OBJECTIVES
The purpose of this study was to inspect the clinical characteristics, surgical approaches, functional preservation, and complications of petrous bone cholesteatoma and to propose appropriate surgical approaches based on long-term follow-up cases and previous reports in the literature.
METHODS
The medical records of 31 patients who underwent surgery for petrous bone cholesteatoma between 1990 and 2011 at two tertiary referral hospitals were retrospectively analyzed with regard to the classification, type of surgical approach, preservation of facial and auditory function, and recurrence.
RESULTS
Of 31 cases, 16 were supralabyrinthine (class I), 1 was infralabyrinthine-apical (class III), 13 were massive (class IV), and 1 was apical (class V). Facial nerve palsy was found in 35.5% of the cases (11 cases). Hearing was preserved in 11 of 22 patients who had better than a 50-dB hearing level of bone conduction pure tone average preoperatively. Preoperative hearing was preserved in only four of the patients in class I (supralabyrinthine). Facial function was preserved or improved in 29 patients (93.5%).
CONCLUSION
Complete removal of cholesteatoma of petrous bone can be achieved by choosing the appropriate approach based on location and extent. Facial function was preserved postoperatively in most reviewed cases. Auditory function could not be preserved postoperatively in some cases, but preserving residual hearing levels can be accomplished mostly in supralabyrinthine cholesteatomas with the appropriate surgical approach.
Keyword
MeSH Terms
Figure
-
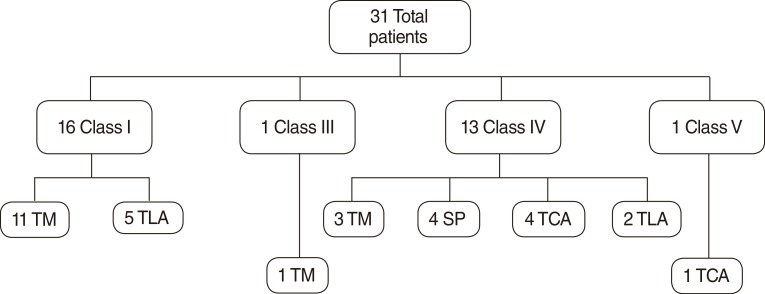
Fig. 1 Surgical approaches used to treat 31 petrous bone cholesteatomas classified according to the Sanna classification. TM, tympanomastoidectomy; TLA, translabyrinthine approach; SP, subtotal petrosectomy; TCA, transcochlear approach.
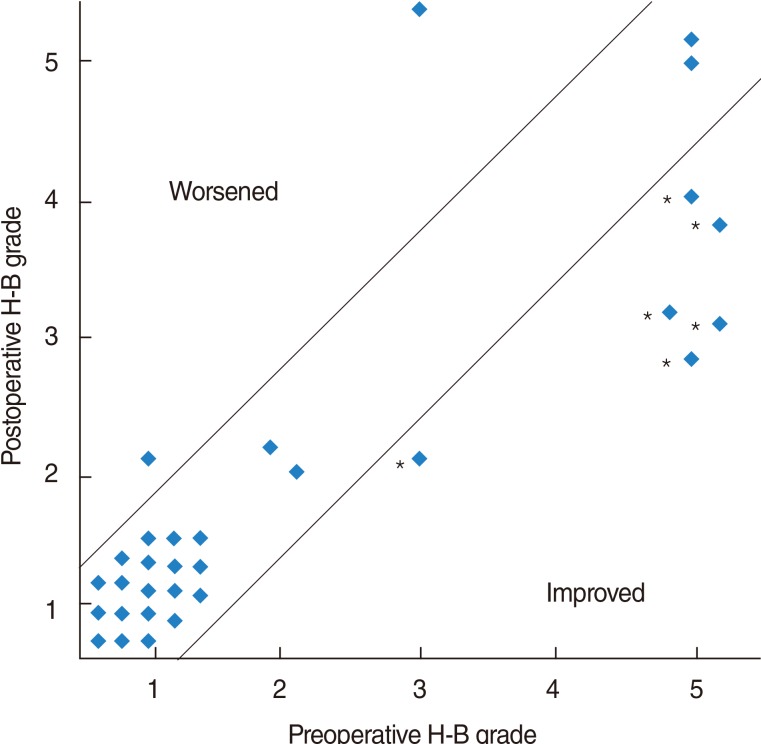
Fig. 2 Comparison of pre- and postoperative facial nerve function according to the House-Brackmann (H-B) grading system. Facial function was improved postoperatively in 6 cases (*) but worsen in 2 cases.
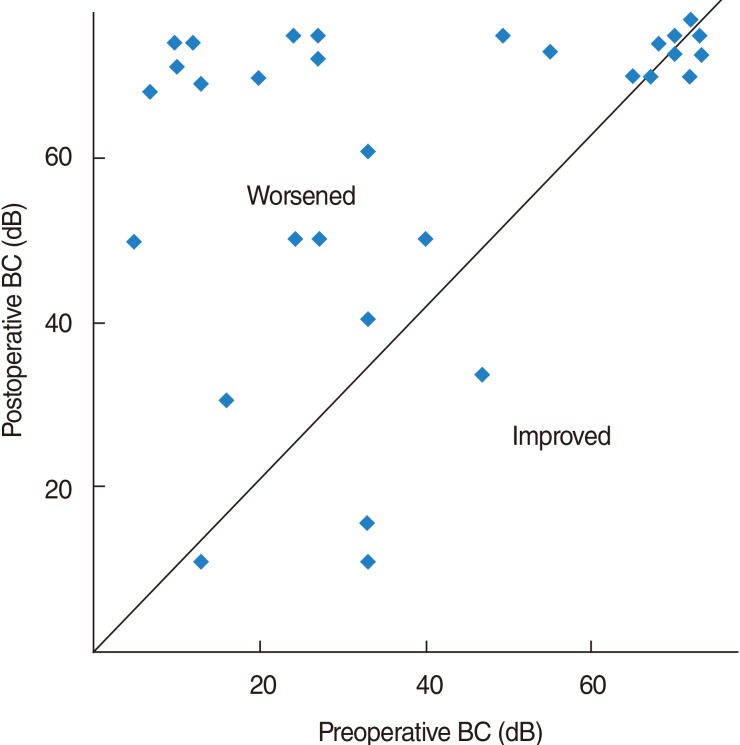
Fig. 3 Comparison of pre- and postoperative hearing levels. Hearing was sacrificed in 11 patients who had residual hearing preoperatively. BC, bone conduction.
Reference
-
1. King TT, Benjamin JC, Morrison AW. Epidermoid and cholesterol cysts in the apex of the petrous bone. Br J Neurosurg. 1989; 3(4):451–461. PMID: 2803593.
Article2. Michaels L. An epidermoid formation in the developing middle ear: possible source of cholesteatoma. J Otolaryngol. 1986; 6. 15(3):169–174. PMID: 3723656.3. Bartels LJ. Facial nerve and medially invasive petrous bone cholesteatomas. Ann Otol Rhinol Laryngol. 1991; 4. 100(4 Pt 1):308–316. PMID: 2018289.
Article4. Sanna M, Zini C, Gamoletti R, Frau N, Taibah AK, Russo A, et al. Petrous bone cholesteatoma. Skull Base Surg. 1993; 10. 3(4):201–213. PMID: 17170912.
Article5. Sanna M, Pandya Y, Mancini F, Sequino G, Piccirillo E. Petrous bone cholesteatoma: classification, management and review of the literature. Audiol Neurootol. 2011; 1. 16(2):124–136. PMID: 20668373.
Article6. House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg. 1985; 4. 93(2):146–147. PMID: 3921901.
Article7. Moffat D, Jones S, Smith W. Petrous temporal bone cholesteatoma: a new classification and long-term surgical outcomes. Skull Base. 2008; 3. 18(2):107–115. PMID: 18769653.
Article8. Jindal M, Riskalla A, Jiang D, Connor S, O'Connor AF. A systematic review of diffusion-weighted magnetic resonance imaging in the assessment of postoperative cholesteatoma. Otol Neurotol. 2011; 10. 32(8):1243–1249. PMID: 21921855.
Article9. House F, Hitselberger WE. The middle fossa approach for removal of small acoustic tumors. Acta Otolaryngol. 1969; 4. 67(4):413–427. PMID: 5371324.
Article10. Yanagihara N, Nakamura K, Hatakeyama T. Surgical management of petrous apex cholesteatoma: a therapeutic scheme. Skull Base Surg. 1992; 1. 2(1):22–27. PMID: 17170877.11. House WF, De la, Hitselberger WE. Surgery of the skull base: transcochlear approach to the petrous apex and clivus. Otolaryngology. 1978; Sep-Oct. 86(5):ORL-770–ORL-779.
Article12. House WF, Hitselgerger WE. The transcochlear approach to the skull base. Arch Otolaryngol. 1976; 6. 102(6):334–342. PMID: 1084148.
Article13. Chen JM, Fisch U. The transotic approach in acoustic neuroma surgery. J Otolaryngol. 1993; 10. 22(5):331–336. PMID: 8283500.14. Sanna M, De Donato G, Taibah A, Russo A, Falcioni M, Mancini F. Infratemporal fossa approaches to the lateral skull base. Keio J Med. 1999; 12. 48(4):189–200. PMID: 10638143.
Article15. Zanation AM, Snyderman CH, Carrau RL, Gardner PA, Prevedello DM, Kassam AB. Endoscopic endonasal surgery for petrous apex lesions. Laryngoscope. 2009; 1. 119(1):19–25. PMID: 19117306.
Article16. Axon PR, Fergie N, Saeed SR, Temple RH, Ramsden RT. Petrosal cholesteatoma: management considerations for minimizing morbidity. Am J Otol. 1999; 7. 20(4):505–510. PMID: 10431894.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Facial Nerve Paralysis in Patients With Chronic Ear Infections: Surgical Outcomes and Radiologic Analysis
- A Case of Huge Congenital Cholesteatoma of Petrous Apex Treated With Translabyrinthine Marsupialization
- Surgical Anatomy for the Infracochlear Approach to the Petrous Apex
- Factors Contributing to the Facial Paralysis after Temporal Petrous Fractures
- A Case of Thyroid Follicular Carcinoma Metastatic to the Petrous Bone
