Korean J Obstet Gynecol.
2010 Jul;53(7):626-632. 10.5468/kjog.2010.53.7.626.
Clinical characteristics of women with Mullerian anomaly: Twenty years of experience at Asan Medical Center
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Asan Medical Center, Ulsan University College of Medicine, Seoul, Korea. hdchae@amc.seoul.kr
- 2Department of Obstetrics and Gynecology, Inje University College of Medicine, Haeundae Paik Hospital, Busan, Korea.
- KMID: 2273943
- DOI: http://doi.org/10.5468/kjog.2010.53.7.626
Abstract
OBJECTIVE
To investigate the clinical characteristics and reproductive outcomes of women with Mullerian anomalies.
METHODS
One hundred and eighty-six patients were diagnosed with Mullerian anomalies at the Asan Medical Center from 1990 to 2009 and their clinical characteristics and reproductive outcomes were analyzed. Mullerian anomalies were categorized according to the classification by the American Fertility Society (1988).
RESULTS
Mullerian anomaly was noticed in 1 in 1,326 patients (0.075%). Most cases were found in adulthood (84.9%) whereas only 15.1% cases in adolescent or pediatric period. More than 40% of cases were asymptomatic and found incidentally but others suffered from amenorrhea (12.4%), dysmenorrhea (10.8%), abnormal menstruation (10.2%), etc. Most common type of uterine anomalies was uterine didelphys (30.6%), followed by bicornuate uterus (19.4%), Mayer-Rokitansky-Kuster-Hauser syndrome (10.8%), septate uterus (9.1%) and unicornuate uterus (8.6%). On the reproductive outcomes of 251 pregnancies identified, spontaneous miscarriages and preterm labor were quite common (55.8%), and the overall live birth rate was 48.6%. When each anomaly was individually analyzed, the live birth rate was 60.0% in the arcuate uterus and 58.0% in the uterine didelphys. The unicornuate and bicornuate uterus presented a similar chance of having a living child (42.1%, 46.7%), while the septate uterus showed a relatively lower live birth rate (32.4%).
CONCLUSION
Although most cases of Mullerian anomalies are diagnosed in adulthood, many patients may suffer from menstrual abnormalities, dysmenorrhea or recurrent miscarriages since adolescence. The reproductive outcomes of the arcuate uterus and uterine didelphys were better, while those of septate uterus were poor in our study.
Keyword
MeSH Terms
-
Abnormalities, Multiple
Abortion, Habitual
Abortion, Spontaneous
Adolescent
Amenorrhea
Child
Dysmenorrhea
Female
Fertility
Humans
Kidney
Live Birth
Menstruation
Mullerian Ducts
Obstetric Labor, Premature
Pregnancy
Somites
Spine
Urogenital Abnormalities
Uterus
Vagina
Abnormalities, Multiple
Kidney
Mullerian Ducts
Somites
Spine
Urogenital Abnormalities
Uterus
Vagina
Figure
-
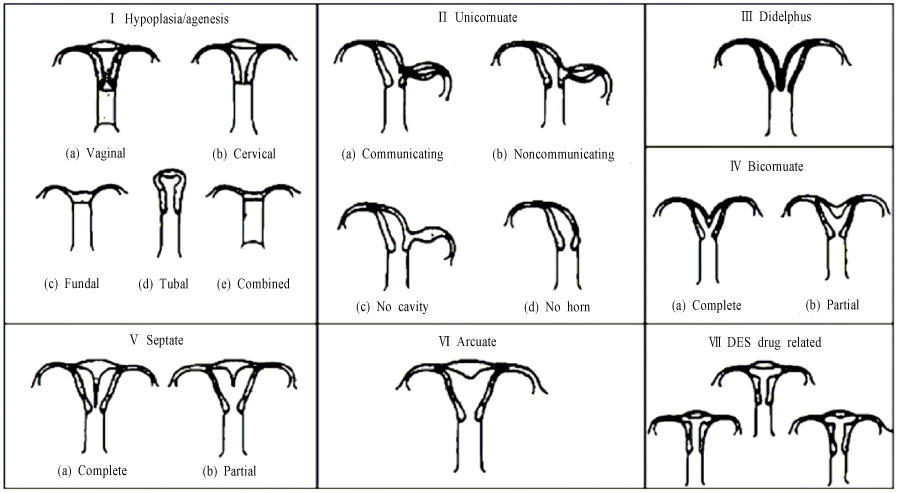
Fig. 1 American Fertility Society (AFS) classification system for Müllerian anomalies (1988). DES: diethylstilbestrol.
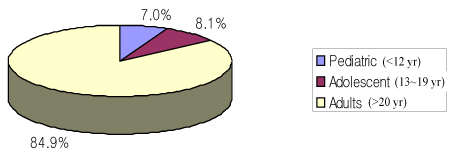
Fig. 2 Diagnostic timing in Müllerian anomalies.
Reference
-
1. Golan A, Langer R, Bukovsky I, Caspi E. Congenital anomalies of the mullerian system. Fertil Steril. 1989. 51:747–755.2. Green LK, Harris RE. Uterine anomalies. Frequency of diagnosis and associated obstetric complications. Obstet Gynecol. 1976. 47:427–429.3. Heinonen PK, Saarikoski S, Pystynen P. Reproductive performance of women with uterine anomalies. An evaluation of 182 cases. Acta Obstet Gynecol Scand. 1982. 61:157–162.4. Simon C, Martinez L, Pardo F, Tortajada M, Pellicer A. Mullerian defects in women with normal reproductive outcome. Fertil Steril. 1991. 56:1192–1193.5. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, mullerian anomalies and intrauterine adhesions. Fertil Steril. 1988. 49:944–955.6. Rock JA. Anomalous development of the vagina. Semin Reprod Endocrinol. 1986. 4:13–31.7. Kim HS, Kim JG, Moon SY, Lee JY, Chang YS. Reproductive performance of women with uterine anomalies. Korean J Fertil Steril. 1986. 13:137–144.8. Kim HJ, Shin HM, Song JY, Kim SY, Chung JE, Kwon DJ, et al. Clinical characteristics of 110 women with uterine anomalies. Korean J Obstet Gynecol. 2008. 51:1472–1480.9. Jung KS, Yoo JO, Cho HS, Woo BH, Kang SM. The congenitial uterine or vaginal anomalies (39 cases) and obstetrical problems. Korean J Obstet Gynecol. 1983. 26:904–911.10. Baik NG, Kim IB, Kwon DJ, Park TC, Lee JW, Kim SP. Clinical study of women with uterine anomalies. Korean J Obstet Gynecol. 1995. 38:1848–1853.11. Kelley JL 3rd, Edwards RP, Wozney P, Vaccarello L, Laifer SA. Magnetic resonance imaging to diagnose a mullerian anomaly during pregnancy. Obstet Gynecol. 1990. 75:521–523.12. Rackow BW, Arici A. Reproductive performance of women with mullerian anomalies. Curr Opin Obstet Gynecol. 2007. 19:229–237.13. Raga F, Bauset C, Remohi J, Bonilla-Musoles F, Simon C, Pellicer A. Reproductive impact of congenital Mullerian anomalies. Hum Reprod. 1997. 12:2277–2281.14. Semmens JP. Congenital anomalies of female genital tract. Functional classification based on review of 56 personal cases and 500 reported cases. Obstet Gynecol. 1962. 19:328–350.15. Tulandi T, Arronet GH, McInnes RA. Arcuate and bicornuate uterine anomalies and infertility. Fertil Steril. 1980. 34:362–364.16. Musich JR, Behrman SJ. Obstetric outcome before and after metroplasty in women with uterine anomalies. Obstet Gynecol. 1978. 52:63–66.17. Rock JA, Jones HW Jr. The clinical management of the double uterus. Fertil Steril. 1977. 28:798–806.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adenomyotic cyst mimicking a congenital Müllerian anomaly: Diagnosis and treatment with laparoscopy
- Diagnosis and current treatment of Mullerian duct anomaly
- Currarino triad with Mullerian duct anomaly in mother and daughter without MNX1 gene mutation
- Three cases of successful pregnancy outcome after intensive care in the patients with complete uterine septum, cervical duplication and longitudinal vaginal septum
- CT and MRI findings of vixed mullerian tumor: report of three cases
