Brain Neurorehabil.
2012 Sep;5(2):52-57. 10.12786/bn.2012.5.2.52.
Endocrinologic Complications after Traumatic Brain Injury
- Affiliations
-
- 1Department of Rehabilitation Medicine, Seoul National University College of Medicine, Korea. keepwiz@gmail.com
- KMID: 2270740
- DOI: http://doi.org/10.12786/bn.2012.5.2.52
Abstract
- The endocrinologic complications such as adrenal insufficiency and hypopituitarism are common after traumatic brain injury (TBI) portending poor rehabilitation outcome. Anterior pituitary dysfunction presents as hypothyroidism, hypogonadism, growth hormone deficiency, adrenal insufficiency and hyperprolactinemia, whereas posterior pituitary dysfunction includes syndrome of inappropriate antidiuretic hormone and central diabetes insipidus. Careful history taking and physical examination are essential to detect these abnormalities early. Laboratory tests such as serum/urine sodium and osmolality, thyroid hormone, testosterone, estradiol, cortisol, prolactin, growth hormone or IGF-1 are also necessary. Screening of endocrinologic functions is recommended especially in patients with moderate or severe TBI, skull base fracture or diffuse axonal injury 3 to 6 months after injury. Further studies are needed to reveal the effect of early correction of endocrinologic abnormality on long-term functional outcome.
MeSH Terms
-
Adrenal Insufficiency
Brain Injuries
Diabetes Insipidus, Neurogenic
Diffuse Axonal Injury
Endocrine System Diseases
Estradiol
Growth Hormone
Humans
Hydrocortisone
Hyperprolactinemia
Hypogonadism
Hypopituitarism
Hypothyroidism
Insulin-Like Growth Factor I
Mass Screening
Osmolar Concentration
Physical Examination
Prolactin
Skull Base
Sodium
Testosterone
Thyroid Gland
Treatment Outcome
Estradiol
Growth Hormone
Hydrocortisone
Insulin-Like Growth Factor I
Prolactin
Sodium
Testosterone
Figure
-
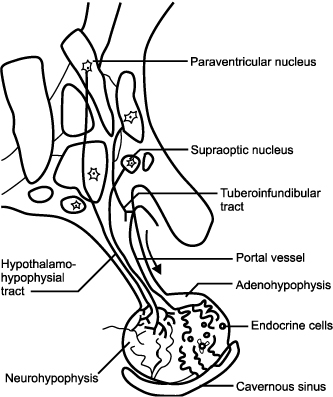
Fig. 1 Hypothalamus and pituitary gland.

Fig. 2 The prevalence of anterior hypopituitarism in survivors of traumatic brain injury.8 1: Lieberman et al,16 2: Aimaretti et al,17 3: Popovic et al,18 4: Leal-Cerro et al,19 5: Aimaretti et al,20 6A: Schneider et al (3 months after injury),21 6B: Schneider et al (12 months after injury),21 7A: Tanriverdi et al (24 hours after injury),22 7B: Tanriverdi et al (12 months after injury),22 8: Klose et al,23 GHD: Growth hormone deficiency, ACTHD: Adrenocorticotrophic hormone deficiency, GnTD: Gonadotropin deficiency, TSHD: Thyroid-stimulating hormone deficiency, PRL: Prolactin.
Reference
-
1. FitzGerald MJT, Gruener G, Mtui E. Clinical Neuroanatomy and Neuroscience. 2006. Saunders.2. Standring S, Gray H. Gray's Anatomy: the Anatomical Basis of Clinical Practice. 2008. 40th ed. Edinburgh: Churchill Livingstone/Elsevier.3. Kornblum RN, Fisher RS. Pituitary lesions in craniocerebral injuries. Arch Pathol. 1969. 88:242–248.4. Crompton MR, Layton DD. Delayed radionecrosis of the brain following therapeutic x-radiation of the pituitary. Brain. 1961. 84:85–101.5. Ceballos R. Pituitary changes in head trauma (analysis of 102 consecutive cases of head injury). Ala J Med Sci. 1966. 3:185–198.6. L'Vovich AI. Descending pathways of the frontal lobe cortex to nuclei of the hypothalamic mamillary bodies in craniocerebral trauma in humans. Neurosci Behav Physiol. 2001. 31:371–374.7. Kokshoorn NE, Wassenaar MJ, Biermasz NR, Roelfsema F, Smit JW, Romijn JA, Pereira AM. Hypopituitarism following traumatic brain injury: prevalence is affected by the use of different dynamic tests and different normal values. Eur J Endocrinol. 2010. 162:11–18.8. Behan LA, Phillips J, Thompson CJ, Agha A. Neuroendocrine disorders after traumatic brain injury. J Neurol Neurosurg Psychiatry. 2008. 79:753–759.9. Benvenga S, Campenni A, Ruggeri RM, Trimarchi F. Clinical review 113: Hypopituitarism secondary to head trauma. J Clin Endocrinol Metab. 2000. 85:1353–1361.10. Schneider M, Schneider HJ, Yassouridis A, Saller B, von Rosen F, Stalla GK. Predictors of anterior pituitary insufficiency after traumatic brain injury. Clin Endocrinol (Oxf). 2008. 68:206–212.11. Agha A, Phillips J, O'Kelly P, Tormey W, Thompson CJ. The natural history of post-traumatic hypopituitarism: implications for assessment and treatment. Am J Med. 2005. 118:1416.12. Niederland T, Makovi H, Gál V, Andréka B, Ábrahám CS, Kovács J. Abnormalities of pituitary function after traumatic brain injury in children. J Neurotrauma. 2007. 24:119–127.13. Agha A, Rogers B, Sherlock M, O'Kelly P, Tormey W, Phillips J, Thompson CJ. Anterior pituitary dysfunction in survivors of traumatic brain injury. J Clin Endocrinol Metab. 2004. 89:4929–4936.14. Bancroft J. The endocrinology of sexual arousal. J Endocrinol. 2005. 186:411–427.15. Sambandam K, Vijayan A. Cooper DH, Krainik AJ, Lubner SJ, Reno HEL, editors. Fluid and Electrolyte Management. The Washington Manual of Medical Therapeutics. 2007. 32nd ed. Lippincott Williams & Wilkins;54–101.16. Lieberman SA, Oberoi AL, Gilkison CR, Masel BE, Urban RJ. Prevalence of neuroendocrine dysfunction in patients recovering from traumatic brain injury. J Clin Endocrinol Metab. 2001. 86:2752–2756.17. Aimaretti G, Ambrosio MR, Di Somma C, Fusco A, Cannavò S, Gasperi M, Scaroni C, De Marinis L, Benvenga S, degli Uberti EC, Lombardi G, Mantero F, Martino E, Giordano G, Ghigo E. Traumatic brain injury and subarachnoid haemorrhage are conditions at high risk for hypopituitarism: screening study at 3 months after the brain injury. Clin Endocrinol (Oxf). 2004. 61:320–326.18. Popovic V, Pekic S, Pavlovic D, Maric N, Jasovic-Gasic M, Djurovic B, Medic Stojanoska M, Zivkovic V, Stojanovic M, Doknic M, Milic N, Djurovic M, Dieguez C, Casanueva FF. Hypopituitarism as a consequence of traumatic brain injury (TBI) and its possible relation with cognitive disabilities and mental distress. J Endocrinol Invest. 2004. 27:1048–1054.19. Leal-Cerro A, Flores JM, Rincon M, Murillo F, Pujol M, Garcia-Pesquera F, Dieguez C, Casanueva FF. Prevalence of hypopituitarism and growth hormone deficiency in adults long-term after severe traumatic brain injury. Clin Endocrinol (Oxf). 2005. 62:525–532.20. Aimaretti G, Ambrosio MR, Di Somma C, Gasperi M, Cannavò S, Scaroni C, Fusco A, Del Monte P, De Menis E, Faustini-Fustini M, Grimaldi F, Logoluso F, Razzore P, Rovere S, Benvenga S, Degli Uberti EC, De Marinis L, Lombardi G, Mantero F, Martino E, Giordano G, Ghigo E. Residual pituitary function after brain injury-induced hypopituitarism: a prospective 12-month study. J Clin Endocrinol Metab. 2005. 90:6085–6092.21. Schneider HJ, Schneider M, Saller B, Petersenn S, Uhr M, Husemann B, von Rosen F, Stalla GK. Prevalence of anterior pituitary insufficiency 3 and 12 months after traumatic brain injury. Eur J Endocrinol. 2006. 154:259–265.22. Tanriverdi F, Senyurek H, Unluhizarci K, Selcuklu A, Casanueva FF, Kelestimur F. High risk of hypopituitarism after traumatic brain injury: a prospective investigation of anterior pituitary function in the acute phase and 12 months after trauma. J Clin Endocrinol Metab. 2006. 91:2105–2111.23. Klose M, Juul A, Poulsgaard L, Kosteljanetz M, Brennum J, Feldt-Rasmussen U. Prevalence and predictive factors of post-traumatic hypopituitarism. Clin Endocrinol (Oxf). 2007. 67:193–201.
