Shoulder Joint Infectious Arthritis and Acromioclavicular Joint Osteomyelitis due to Candida
- Affiliations
-
- 1Department of Rehabilitation Medicine, Inje University, College of Medicine, Ilsan Paik Hospital, Goyang 411-706, Korea. remedios1004@naver.com
- 2Department of Internal Medicine, Inje University, College of Medicine, Ilsan Paik Hospital, Goyang 411-706, Korea.
- KMID: 2266732
- DOI: http://doi.org/10.5535/arm.2012.36.4.573
Abstract
- Candida species inhabit the skin and mucous membranes of healthy individuals with low virulence, and osteomyelitis due to candida is very rare. However, the incidence of invasive candidal infection caused by intravenous drug use, broad-spectrum antibiotics, and indwelling central venous catheter is increasing. A 73-year old man visited the outpatient clinic complaining of right shoulder pain that radiated to the right acromioclavicular joint. He had undergone multiple injection procedures followed by nonsteroidal anti-inflammatory drug therapy for several weeks. The ultrasonographic findings showed a heterogeneous mass around the right acromioclavicular joint, while the right shoulder MRI and the overall findings of the body bone scan were suggestive of osteomyelitis. Pathologic findings of ultrasonographically guided joint aspiration fluid showed acute and chronic nonspecific inflammation, while the tissue culture and staining revealed Candida parapsilosis.
Keyword
MeSH Terms
Figure
-
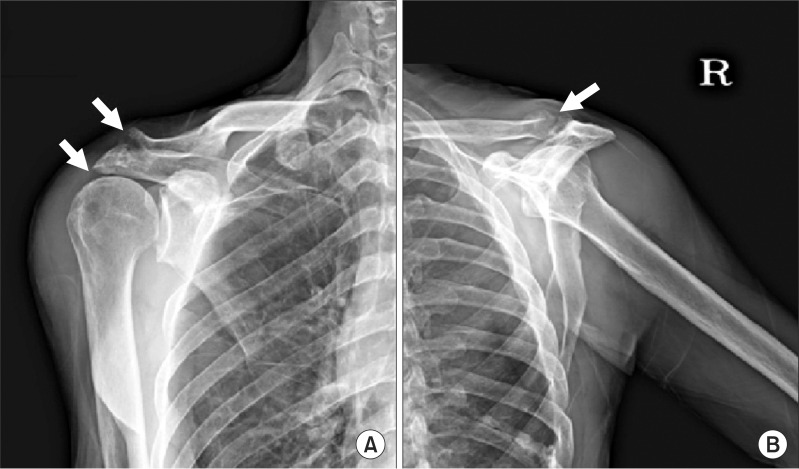
Fig. 1 (A) Anteroposterior radiograph of the right shoulder shows markedly erosive and sclerotic changes in the acromioclavicular joint, and joint space narrowing in the acromiohumeral joint. (B) Y-view radiograph of the right shoulder shows markedly erosive and sclerotic changes in the acromioclavicular joint.

Fig. 2 Whole body bone scan with Tc-99m DPD shows increased radioisotope uptake in the acromial area of the right shoulder.
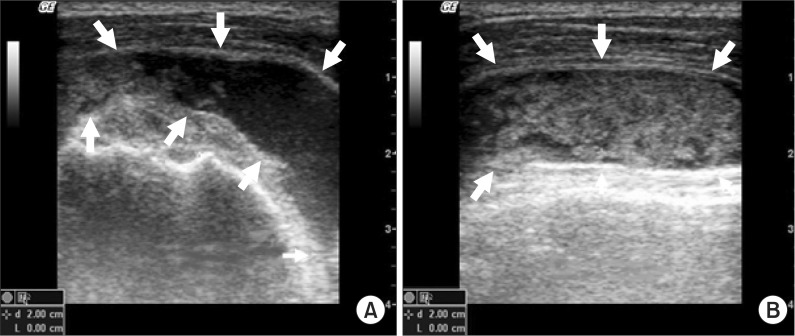
Fig. 3 (A) Short-axis ultrasonographic image of the right humeral head shows a heterogeneous cystic mass around the subacromial bursa. (B) Long-axis ultrasonographic image of the right humeral head shows a heterogeneous cystic mass over the biceps tendon.
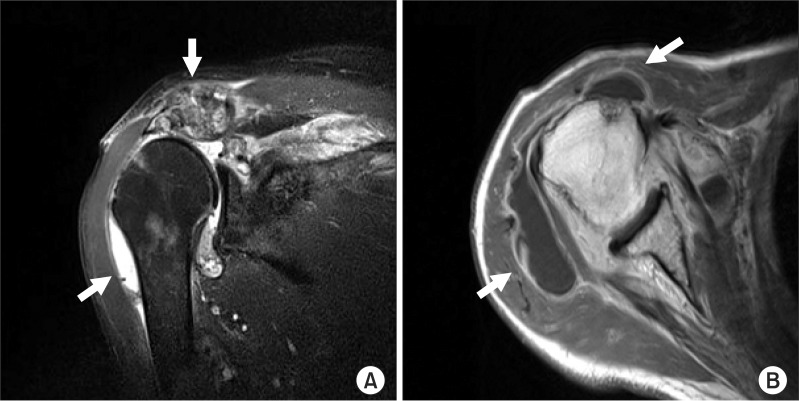
Fig. 4 (A) Transverse T2 weighted magnetic resonance imaging demonstrates joint erosion with osteomyelitis of the acromioclavicular joint and right shoulder joint. (B) Coronal T1 weighted magnetic resonance imaging shows a rim-enhancing lesion in the right shoulder joint compatible with right shoulder joint infectious arthritis.
Reference
-
1. Waldvogel FA, Papageorgiou PS. Osteomyelitis: the past decade. N Engl J Med. 1980; 303:360–370. PMID: 6993944.
Article3. Arias F, Meta-Essayag S, Landaeta ME, Capriles CH, Perez C, Nunez MJ, Carvajal A, Silva M. Candida albicans osteomyelitis: case report and literature review. Int J Infect Dis. 2004; 8:307–314. PMID: 15325600.
Article4. Kim HJ, Lee JC, Shin BA, Song HY. The Korean society for microbiology textbook of medical microbiology. 2005. 4th ed. Killiney: Elsevier Pte Ltd;p. 669–676.5. Edmond MB, Wallace SE, McClish DK, Pfaller MA, Jones RN, Wenzel RP. Nosocomial bloodstream infections in United States hospitals: a three-year analysis. Clin Infect Dis. 1999; 29:239–244. PMID: 10476719.
Article6. Cone LA, Byrd RG, Potts BE, Wuesthoff M. Diagnosis and treatment of Candida vertebral osteomyelitis: clinical experience with a short course therapy of amphotericin B lipid complex. Surg Neurol. 2004; 62:234–237. PMID: 15336867.
Article7. Petrikkos G, Skiada A, Sabatakou H, Antoniadou A, Dosios T, Giamarellou H. Case report. Successful treatment of two cases of post-surgical sternal osteomyelitis, due to Candida krusei and Candida albicans, respectively, with high doses of triazoles (fluconazole, itraconazole). Mycoses. 2001; 44:422–425. PMID: 11766111.8. Seok H, Kim SH, Kim DH, Kim TH, Kim HK. Cervical osteomyelitis and radiculopathy due to Candida: a case report. J Korean Acad Rehabil Med. 2007; 31:482–485.9. Pennisi AK, Davis DO, Wiesel S, Moskovitz P. CT appearance of Candida diskitis. J Comput Assist Tomogr. 1985; 9:1050–1054. PMID: 4056136.
Article10. Kim DH, Lee JA, Jo HS, Park KR, Park JD, Kim BI, Choi JH. Systemic candidiasis in neonatal intensive care unit: a 8-year experience. J Korean Soc Neonatol. 2001; 8:33–45.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acromioclavicular Septic Arthritis and Sternoclavicular Septic Arthritis with Contiguous Pyomyositis
- The Treatment of Grade 3 Acute Acromioclavicular Joint Injuries with Modified Neviaser Technique
- Candida Arthritis in a Hemodialysis Patient
- Arthroscopic Treatment of Septic Arthritis of Acromioclavicular Joint
- Candida Septic Arthritis with Rice Body Formation: A Case Report and Review of Literature
