Arthroscopic Treatment of Septic Arthritis of Acromioclavicular Joint
- Affiliations
-
- 1Department of Orthopedic Surgery, Kangnam Sacred Heart Hospital, College of Medicine, Hallym University, Seoul, Korea. chungkjmd@dreamwiz.com
- 2Department of Radiology, Hallym University Sacred Heart Hospital, College of Medicine, Hallym University, Seoul, Korea.
- KMID: 999439
- DOI: http://doi.org/10.4055/cios.2010.2.3.186
Abstract
- Septic arthritis requires an early diagnosis and proper treatment to prevent the destruction of articular cartilage and joint contracture. This paper presents a rare case of septic arthritis of the acromioclavicular joint that was treated with arthroscopic debridement and resection of the distal clavicle.
Keyword
MeSH Terms
Figure
-
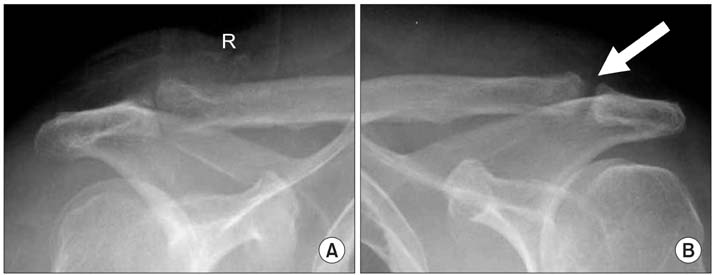
Fig. 1 Plain radiography of the right (A) and left (B) acromioclavicular (AC) joint. The left AC joint (B) shows joint space widening relative to unaffected right AC joint (A). The joint margin of the left AC joint shows periarticular bone erosions.
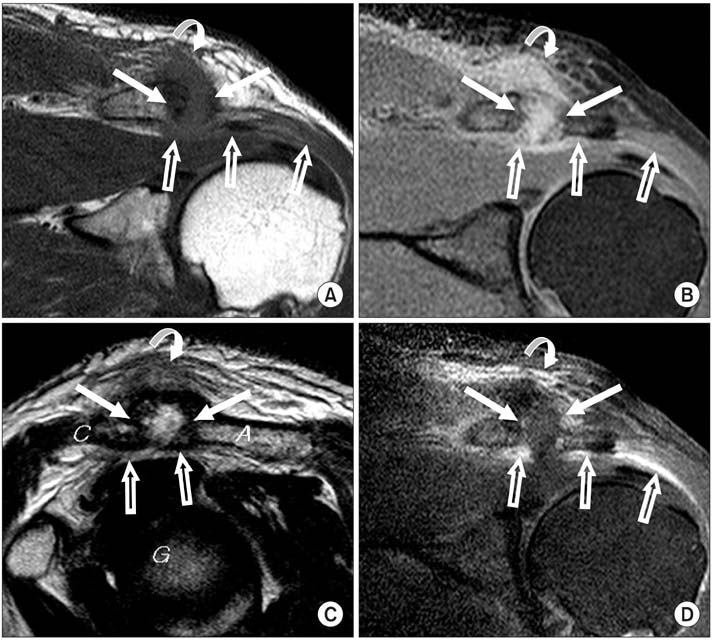
Fig. 2 MR images of the left shoulder. (A) T1-weighted image oblique coronal scan shows periarticular bone erosions and joint space widening of the acromioclavicular (AC) joint (arrows). The AC joint shows isosignal intensity relative to the muscle. Periarticular soft tissue shows low signal intensity relative to the adjacent normal fat tissue (curved arrow). The subacromial and subdeltoid space shows low signal intensity relative to the normal fat tissue (open arrows). (B) Fat suppressed proton density weighted image oblique coronal scan shows periarticular bone erosions and joint space widening of the AC joint (arrows). The AC joint shows high intensity relative to the muscle. Periarticular soft tissue shows high signal intensity relative to the adjacent normal fat tissue (curved arrow). The subacromial and subdeltoid space shows high signal intensity relative to the normal fat tissue (open arrows). (C) The T2-weighted image obique sagittal scan show periarticular bone erosions and widening of the AC joint space (arrows). The AC joint shows heterogenous high intensity relative to the muscle. The periarticular soft tissue shows high signal intensity relative to the adjacent normal fat tissue (curved arrow). The subacromial and subdeltoid space shows heterogenous low signal intensity relative to normal fat tissue (open arrows). (D) Fat suppressed Gd-enhancement T1-weighted image oblique coronal scan shows joint space widening (arrows). Periarticular bone marrow and periarticular soft tissue (curved arrow) shows heterogenous contrast enhancement. Subacromial-subdeltoid bursa shows diffuse thickening and contrast enhancement (open arrows). A: Acromion, C: Clavicle, G: Glenoid.
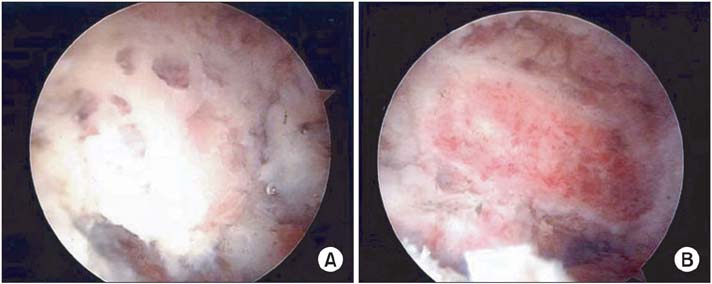
Fig. 3 Arthroscopic views show a multiple subchondral punched out bony lesion of the acromioclavicular joint (A) and postoperative findings of arthroscopic debridement and distal clavicle resection (B).

Fig. 4 There is no clavicle elevation of the left acromioclavicular joint on the 2 year follow-up X-ray after arthroscopic debridement and distal clavicle resection.
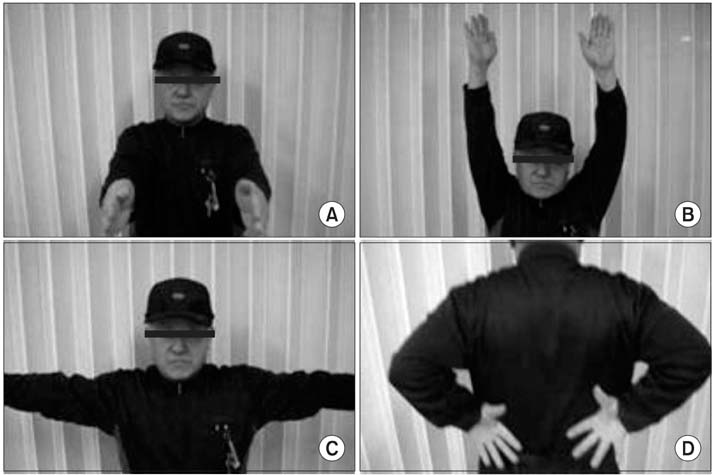
Fig. 5 The patient shows a good range of motion on the left shoulder at the 2 year follow-up.
Cited by 1 articles
-
Pharmacologic treatment of osteoarthritis
Seung-Hoon Baek, Shin-Yoon Kim
J Korean Med Assoc. 2013;56(12):1123-1131. doi: 10.5124/jkma.2013.56.12.1123.
Reference
-
1. Bremell T, Abdelnour A, Tarkowski A. Histopathological and serological progression of experimental Staphylococcus aureus arthritis. Infect Immun. 1992. 60(7):2976–2985.
Article2. Adams R, McDonald M. Cryptococcal arthritis of the acromio-clavicular joint. N C Med J. 1984. 45(1):23–24.3. Sobrino J, Bosch X, Wennberg P, Villalta J, Grau JM. Septic arthritis secondary to group C streptococcus typed as Streptococcus equisimilis. J Rheumatol. 1991. 18(3):485–486.4. Chirag AS, Ropiak CR, Bosco Iii JA, Egol KA. Septic arthritis of the acromioclavicular joint: a report of four cases. Bull NYU Hosp Jt Dis. 2007. 65(4):308–311.5. Park AL, Dlabach JA. Canale ST, editor. Infectious arthritis. Campbell's operative orthopaedics. 2003. St. Louis: Mosby;685–711.6. Tan V, Pepe MD, Esterhai JL Jr. Iannotti JP, Williams GR, editors. Sepsis of the shoulder girdle. Disorders of the shoulder: diagnosis and management. 1999. Philadelphia: Lippincott Williams & Wilkins;951–973.7. Resnick D. Bone and joint imaging. 1996. 2nd ed. Philadelphia: WB Saunders.8. Widman DS, Craig JG, van Holsbeeck MT. Sonographic detection, evaluation and aspiration of infected acromio-clavicular joints. Skeletal Radiol. 2001. 30(7):388–392.
Article9. Nelson MC, Leather GP, Nirschl RP, Pettrone FA, Freedman MT. Evaluation of the painful shoulder: a prospective comparison of magnetic resonance imaging, computerized tomographic arthrography, ultrasonography, and operative findings. J Bone Joint Surg Am. 1991. 73(5):707–716.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Arthroscopic Treatment of Septic Arthritis of the Hip in a Child: A Case Report
- Treatment of the Septic Arthritis in Shoulder Joint after Arthroscopic Rotator Cuff Repair
- Arthroscopic Treatment of Acromioclavicular Joint Dislocations
- Acromioclavicular Septic Arthritis and Sternoclavicular Septic Arthritis with Contiguous Pyomyositis
- Arthroscopic Treatment for Septic Arthritis of the Shoulder in Neonates
