Korean Circ J.
2007 Mar;37(3):119-126. 10.4070/kcj.2007.37.3.119.
Association of New Parameters Derived from Relation between RR intervals and Left Ventricular Performances with Heart Failure in Patients with Atrial Fibrillation and Normal Systolic Function
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, College of Medicine, Chung-Ang University, Seoul, Korea. cjkim@cau.ac.kr
- KMID: 2227083
- DOI: http://doi.org/10.4070/kcj.2007.37.3.119
Abstract
-
BACKGROUND AND OBJECTIVES: Heart failure (HF) may occur in atrial fibrillation (AF) patients with a normal left ventricular (LV) systolic function if the diastolic function is impaired. The association of new parameters from the relationship between the preceding RR interval (RR-1) and LV outflow peak ejection velocity (Vpe) with systolic function has been reported. The aim of this study was to observe whether these parameters were associated with HF in AF patients with a normal systolic function.
SUBJECTS AND METHODS
AF patients with a normal systolic function were divided into two groups according to the presence (n=16) or absence (n=30) of a history of HF. From the logarithmic equation between RR-1 and Vpe, the slope, Vpe at RR-1 second (Vpe-1), and Slope/Vpe-1 were calculated.
RESULTS
Patients with a history of HF were older (p=0.037) and tended to more frequently have hypertension (p=0.063) than those with no history of HF. The ejection fractions were similar between the two groups. In the coordinates with RR-1 from 0.6 to 1 second, the slope tended to be steeper (p=0.074) and slope/Vpe-1 was higher in patients with a history of HF (p=0.011). The Vpe-1 was similar between the two groups (p=0.66). A multiple forward logistic regression analysis showed that slope/Vpe-1 was the only independent variable associated with the occurrence of HF. Slope/Vpe-1 was related with aortic regurgitation, HF history, and the interventricular septal thickness in a multiple stepwise regression analysis.
CONCLUSION
New parameters from the relationship between the RR intervals and LV performances were associated with the occurrence of HF in AF patients with a normal systolic function. This finding suggests that these parameters may be related with the LV diastolic function.
Keyword
MeSH Terms
Figure
-
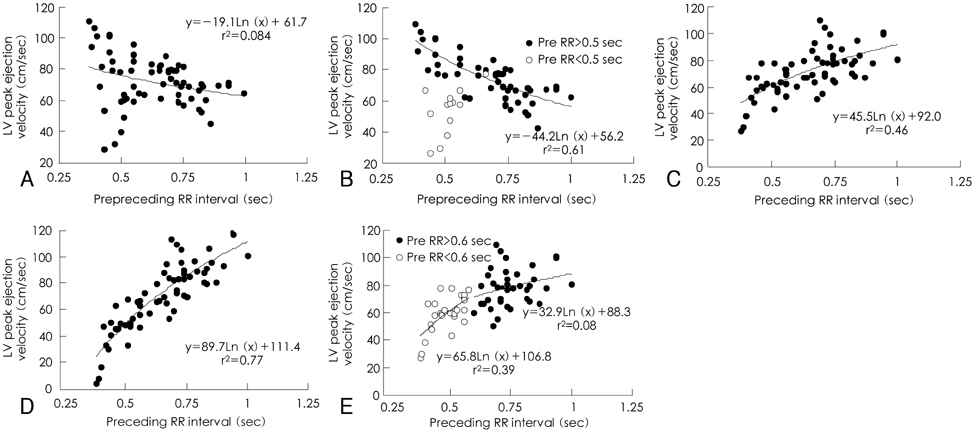
Fig. 1 The representative example of the relationship of preceding (RR-1) and prepreceding RR (RR-2) intervals with left ventricular peak ejection velocity (Vpe). A: relation between RR-2 and Vpe. B: relation between RR-2 and Vpe when the coordinates with RR-1≤0.5 second were excluded. C: relation between RR-1 and Vpe. D: relation between RR-1 and Vpe adjusted with the influence of RR-2. E: relation between RR-1 and Vpe when divided into two zones, short RR intervals (>0.6 second) and long RR interval (>0.6 second) (Adopted from reference 16 with modification). LV: left ventricular.
Reference
-
1. Heist EK, Ruskin JN. Atrial fibrillation and congestive heart failure: risk factors, mechanisms, and treatment. Prog Cardiovasc Dis. 2006. 48:256–269.2. Fuster V, Ryden LE, Asinger RW, et al. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: executive summary. Circulation. 2001. 104:2118–2150.3. Furberg CD, Psaty BM, Manolio TA, Gardin JM, Smith VE, Rautaharju PM. Prevalence of atrial fibrillation in elderly subjects (the Cardiovascular Health Study). Am J Cardiol. 1994. 74:236–241.4. Lee SM, Choe CW, Hong SJ, et al. The joint multicenter study on the atrial fibrillation in Korea. Korean Circ J. 2000. 30:646–652.5. Packer DL, Bardy GH, Worley SJ, et al. Tachycardia-induced cardiomyopathy: a reversible form of left ventricular dysfunction. Am J Cardiol. 1986. 57:563–570.6. Daoud EG, Weiss R, Bahu M, et al. Effect of an irregular ventricular rhythm on cardiac output. Am J Cardiol. 1996. 78:1433–1436.7. Clark DM, Plumb VJ, Epstein AE, Kay GN. Hemodynamic effects of an irregular sequence of ventricular cycle lengths during atrial fibrillation. J Am Coll Cardiol. 1997. 30:1039–1045.8. Effat M, Schick EC, Martin DT, Gaasch WH. Effect of rhythm regularization on left ventricular contractility in patients with atrial fibrillation. Am J Cardiol. 2000. 85:114–116.9. Dubrey SW, Falk RH. Optimal number of beats for the Doppler measurement of cardiac output in atrial fibrillation. J Am Soc Echocardiogr. 1997. 10:67–71.10. Schneider F, Martin DT, Schick EC, Gaasch WH. Interval-dependent changes in left ventricular contractile state in lone atrial fibrillation and in atrial fibrillation associated with coronary artery disease. Am J Cardiol. 1997. 80:586–590.11. Gosselink AT, Blanksma PK, Crijns HJ, et al. Left ventricular beat-to-beat performance in atrial fibrillation: contribution of Frank-Starling mechanism after short rather than long RR intervals. J Am Coll Cardiol. 1995. 26:1516–1521.12. Freeman GL, Colston JT. Evaluation of left ventricular mechanical restitution in closed-chest dogs based on single-beat elastance. Circ Res. 1990. 67:1437–1445.13. Kerr AJ, Simmonds MB, Stewart RA. Influence of heart rate on stroke volume variability in atrial fibrillation in patients with normal and impaired left ventricular function. Am J Cardiol. 1998. 82:1496–1500.14. Rawles JM. A mathematical model of left ventricular function in atrial fibrillation. Int J Biomed Comput. 1988. 23:57–68.15. Pfeiffer KP, Kenner T, Schaefer J. Application of statistical methods for the analysis or interval related cardiac performance variations during cardiac arrhythmia in man. Cardiovasc Res. 1984. 18:80–98.16. Ko HS, Lee KJ, Kim SW, Kim TH, Kim CJ, Ryu WS. Prediction of left ventricular peak ejection velocity by preceding and prepreceding RR intervals in atrial fibrillation: a new method to adjust the influence between two Intervals. J Korean Med Sci. 2002. 17:743–748.17. Ko HS, Kim CJ, Ryu WS. New parameters for left ventricular function in atrial fibrillation: based on the relationship between RR interval and performance. J Korean Med Sci. 2005. 20:20–25.18. Nagahama Y, Schick EC, Gaasch WH. Interval-dependent potentiation of left ventricular contractility is preserved in patients with atrial fibrillation and depressed ejection fraction. Am J Cardiol. 2001. 87:342–346.19. Ha JW, Oh JK. The pathophysiology and diagnostic approaches for diastolic left ventricular dysfunction: a clinical perspective. Korean Circ J. 2005. 35:865–876.20. Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements. Circulation. 1978. 58:1072–1083.21. Ommen SR, Nishimura RA, Appleton CP, et al. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: a comparative simultaneous Doppler-catheterization study. Circulation. 2000. 102:1788–1794.22. Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quinones MA. Doppler tissue imaging: a noninvasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol. 1997. 30:1527–1533.23. Sohn DW, Song JM, Zo JH, et al. Mitral annulus velocity in the evaluation of left ventricular diastolic function in atrial fibrillation. J Am Soc Echocardiogr. 1999. 12:927–931.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- New Parameters for Left Ventricular Function in Atrial Fibrillation: Based on the Relationship between RR Interval and Performance
- Relationship Between RR Intervals and Early Diastolic Mitral Annulus Velocities in Atrial Fibrillation Patients Who do not Have Significant Valvular Diseases
- Relation Between RR Intervals and Early Diastolic Mitral Annular Velocities in Atrial Fibrillation
- Prediction of Left Ventricular Peak Ejection Velocity by Preceding and Prepreceding RR Intervals in Atrial fibrillation:A New Method to Adjust the Influence between Two Intervals
- The Relationship between Preceding RR Intervals and Peak Ejection Velocity of Left Ventricular Outflow in Atrial Fibrillation without Organic Heart Diseases
