Diagnosis of Coronary Restenosis Using Coronary Flow Reserve Measurements Obtained Through Transthoracic Doppler Echocardiography
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. sejoong@yumc.yonsei.ac.kr
- KMID: 2225780
- DOI: http://doi.org/10.4070/kcj.2008.38.6.325
Abstract
-
BACKGROUND AND OBJECTIVES: Coronary flow reserve (CFR) decreases in the presence of significant coronary stenosis. Hence, CFR can be used for the detection of restenosis after percutaneous coronary intervention (PCI). However, because CFR can also be affected by other conditions such as endothelial dysfunction, microvascular damage, and left ventricular hypertrophy, the absolute value of CFR is not routinely used for detection of coronary restenosis. We hypothesized that changes in the value of CFR, rather than the absolute CFR value, are better correlated with restenosis in various clinical settings.
SUBJECTS AND METHODS
We studied 99 patients (71 males/28 females, mean age 58+/-11 years) who underwent successful PCI of the left anterior descending artery. Pre-PCI diagnoses were as follows: 37 unstable angina, 35 stable angina, 27 acute myocardial infarction. CFR using transthoracic Doppler was measured at 48 hours after PCI and at the time of follow-up angiography (6.0+/-1.5 months later). Coronary flow velocity was measured in the distal left anterior descending artery with a 7 MHz transducer (HDI 5,000, Philips, The Netherlands) at baseline and during intravenous infusion of adenosine (140 microgram.kg(-1).min(-1)). Mean diastolic coronary flow velocities from at least three cardiac cycles were averaged.
RESULTS
CFRs in 69 patients without restenosis were 2.55+/-0.99 at 48 hours after PCI and 2.93+/-1.00 at follow-up (p<0.005). CFRs in 30 patients with restenosis (>50% in diameter stenosis) decreased significantly from 2.70+/-1.01 at 48 hours after PCI to 1.98+/-0.91 at follow-up (p<0.001). There was a significant difference in CFR change (ratio of CFR(followup)/CFR(initial)) between the two groups. CFR change had a better receiver operating characteristics (ROC) curve than absolute CFR for prediction of restenosis [area under the curve (AUC) for absolute CFR=0.76, AUC for CFR change=0.82].
CONCLUSION
Restenosis after PCI leads to a significant decrease in CFR, even in the presence of variable baseline CFR values. Serial measurements of CFR can be used to detect restenosis after PCI.
MeSH Terms
-
Adenosine
Angina, Stable
Angina, Unstable
Angiography
Area Under Curve
Arteries
Coronary Restenosis
Coronary Stenosis
Echocardiography
Echocardiography, Doppler
Female
Follow-Up Studies
Humans
Hypertrophy, Left Ventricular
Infusions, Intravenous
Myocardial Infarction
Percutaneous Coronary Intervention
Polyenes
ROC Curve
Transducers
Adenosine
Polyenes
Figure
-
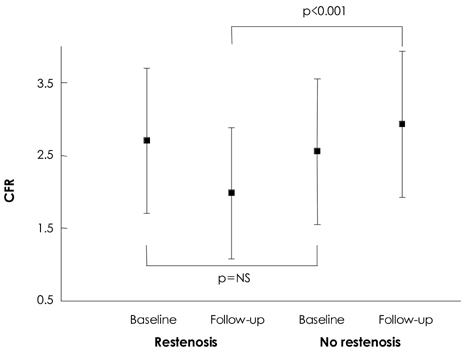
Fig. 1 CFR at baseline and follow-up in patients with restenosis and patients without restenosis. CFRs in 69 patients without restenosis were 2.55±0.99 at 48 hours after PCI and 2.93±1.00 at follow-up (p<0.005). CFRs in 30 patients with restenosis (>50% in diameter stenosis) decreased significantly from 2.70±1.01 to 1.98±0.91 (p<0.001). There was a significant difference of CFR in f/u study between two groups. CFR: coronary flow reserve.
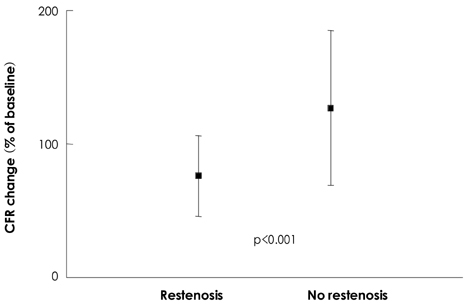
Fig. 2 The change of CFR in patients with restenosis and patients without restenosis. There was a significant difference of CFR change (ratio of CFRf/u/CFRinitial) between two groups. CFR: coronary flow reserve.

Fig. 3 ROC curves for prediction of restenosis using absolute CFR and CFR change. CFR change has better ROC curve than absolute CFR. CFR: coronary flow reserve, AUC: area under the curve, ROC: receiver operating characteristics.
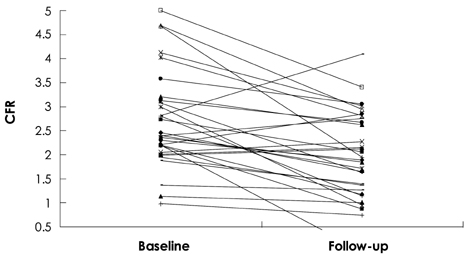
Fig. 4 Serial CFRs in patients with restenosis. In patients with relatively high initial CFR, f/u CFR was still high (>2.0) even with restenosis. CFR: coronary flow reserve.

Fig. 5 Serial CFRs in patients with no restenosis. In patients with relatively low initial CFR, CFR was still low (≤2.0) even without restenosis. CFR: coronary flow reserve.
Reference
-
1. Wilson RF, Marcus ML, White CW. Prediction of the physiologic significance of coronary arterial lesions by quantitative lesion geometry in patients with limited coronary artery disease. Circulation. 1987. 75:723–732.2. Gould KL, Lipscomb K, Hamilton GW. Physiologic basis for assessing critical coronary stenosis: instantaneous flow response and regional distribution during coronary hyperemia as measures of coronary flow reserve. Am J Cardiol. 1974. 33:87–94.3. Gould KL, Lipscomb K. Effects of coronary stenoses on coronary flow reserve and resistance. Am J Cardiol. 1974. 34:48–55.4. Marcus ML, Wright C, Doty D, et al. Measurements of coronary velocity and reactive hyperemia in the coronary circulation of humans. Circ Res. 1981. 49:877–891.5. Weyman AE, Feigenbaum H, Dillon JC, Johnston KW, Eggleton RC. Noninvasive visualization of the left main coronary artery by cross-sectional echocardiography. Circulation. 1976. 54:169–174.6. Fusejima K. Noninvasive measurement of coronary artery blood flow using combined two-dimensional and Doppler echocardiography. J Am Coll Cardiol. 1987. 10:1024–1031.7. Ross JJ Jr, Mintz RG, Chandrasekaran K. Transthoracic two-dimensional high frequency (7.5 MHz) ultrasonic visualization of the distal left anterior descending coronary artery. J Am Coll Cardiol. 1990. 15:373–377.8. Kenny A, Shapiro LM. Transthoracic high-frequency two-dimensional echocardiography, Doppler and color flow mapping to determine anatomy and blood flow patterns in the distal left anterior descending coronary artery. Am J Cardiol. 1992. 69:1265–1268.9. Kenny A, Wisbey CR, Shapiro LM. Measurement of left anterior descending coronary artery flow velocities by transthoracic Doppler ultrasound. Am J Cardiol. 1994. 73:1021–1022.10. Ruscazio M, Montisci R, Colonna P, et al. Detection of coronary restenosis after coronary angioplasty by contrast-enhanced transthoracic echocardiographic Doppler assessment of coronary flow velocity reserve. J Am Coll Cardiol. 2002. 40:896–903.11. Klocke FJ. Measurements of coronary flow reserve: defining pathophysiology versus making decisions about patient care. Circulation. 1987. 76:1183–1189.12. Wilson RF, Laughlin DE, Ackell PH, et al. Transluminal subselective measurement of coronary artery blood flow velocity and vasodilator reserve in man. Circulation. 1985. 72:82–92.13. Clayes MJ, Vrints CJ, Bosmans J, Krug B, Blockx PP, Snoeck JP. Coronary flow reserve during coronary angioplasty in patients with a recent myocardial infarction: relation to stenosis and myocardial viability. J Am Coll Cardiol. 1996. 28:1712–1719.14. Hoffman JI. Maximal coronary flow and the concept of coronary vascular reserve. Circulation. 1984. 70:153–159.15. Marcus ML, Wilson RF, White CW. Methods of measurement of myocardial blood flow in patients: a critical review. Circulation. 1987. 76:245–253.16. Uren NG, Melin JA, De Bruyne B, Wijns W, Baudhuin T, Camici PG. Relation between myocardial blood flow and the severity of coronary artery stenosis. N Engl J Med. 1994. 330:1782–1788.17. Faletra F, Cipriani M, Corno R, et al. Transthoracic high-frequency echocardiographic detection of atherosclerotic lesions in the descending portion of the left coronary artery. J Am Soc Echocardiogr. 1993. 6:290–298.18. Wilson RF, Wyche K, Christiansen BV, Zimmer S, Laxson DD. Effects of adenosine on human coronary circulation. Circulation. 1990. 82:1595–1606.19. Rossen JD, Quillen JE, Lopez AG, Stenberg RG, Talman CL, Winniford MD. Comparison of coronary vasodilation with intravenous dipyridamole and adenosine. J Am Coll Cardiol. 1991. 18:485–491.20. Kern MJ, Deligonul U, Tatineni S, Serota H, Aguirre F, Hilton TC. Intravenous adenosine: continuous infusion and low dose bolus administration for determination of coronary vasodilator reserve in patients with and without coronary artery disease. J Am Coll Cardiol. 1991. 18:718–729.21. Doucette JW, Corl D, Payne GM, et al. Validation of a Doppler guide wire for intravascular measurement of coronary artery flow velocity. Circulation. 1992. 85:1899–1911.22. Hozumi T, Yoshida K, Akasaka T, et al. Noninvasive assessment of coronary flow velocity and coronary flow velocity reserve in the left anterior descending coronary artery by Doppler echocardiography: comparison with invasive technique. J Am Coll Cardiol. 1998. 32:1251–1259.23. Caiati C, Montaldo C, Zedda N, et al. Validation of a new noninvasive method (contrast-enhanced transthoracic second harmonic echo Doppler) for the evaluation of coronary flow reserve: comparison with intracoronary Doppler flow wire. J Am Coll Cardiol. 1999. 34:1193–1200.24. Youn HJ. Demonstration of pathologic coronary flow dynamics using transthoracic doppler echocardiography: its potential role in clinical decision-making. Korean Circ J. 2005. 35:269–281.25. Kim MA, Sohn DW, Cho YS, Kim YJ, Park YB, Choi YS. Changes in coronary flow reserve assessed by transthoracic echocardiography after lipid-lowering therapy in patients with hypercholesterolemia. Korean Circ J. 2004. 34:670–676.26. Sakuma T, Otsuka M, Okimoto T, et al. Optimal time for predicting myocardial viability after successful primary angioplasty in acute myocardial infarction: a study using myocardial contrast echocardiography. Am J Cardiol. 2001. 87:687–692.27. Doo YC, Park SJ, Park SW, et al. Initial results and long-term clinical outcomes after coronary angioplasty. Korean Circ J. 1994. 24:448–457.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Direct Visualization of Coronary Artery and Flow using Transthoracic Doppler Echocardiography
- Demonstration of Pathologic Coronary Flow Dynamics using Transthoracic Doppler Echocardiography: Its Potential Role in Clinical Decision-Making
- Changes in Coronary Flow Reserve Assessed by Transthoracic Echocardiography after Lipid-Lowering Therapy in Patients with Hypercholesterolemia
- Assessment of coronary flow reserve with transthoracic Doppler echocardiography: comparison with intracoronary Doppler method
- Clinical Usefulness of Noninvasive Measurement of Coronary Flow Velocity Reserve with Transthoracic Doppler Echocardiography for Detection of Restenosis after Revascularization of Left Anterior Descending Coronary Artery
