The First Korean Patient With Severe Aortic Stenosis and Bilateral Iliofemoral Artery Disease Treated With Transcatheter Aortic Valve Implantation by Transsubclavian Approach
- Affiliations
-
- 1Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University Health System, Seoul, Korea. mkhong61@yuhs.ac
- 2Department of Thoracic and Cardiovascular Surgery, Severance Cardiovascular Hospital, Yonsei University Health System, Seoul, Korea.
- 3Department of Anesthesiology and Pain Medicine, Severance Cardiovascular Hospital, Yonsei University Health System, Seoul, Korea.
- KMID: 2224984
- DOI: http://doi.org/10.4070/kcj.2012.42.11.796
Abstract
- Transcatheter aortic valve implantation (TAVI) is indicated as an alternative treatment modality to surgical aortic valve replacement for high risk patients. The standard retrograde approach through the femoral artery is not feasible in the case of unfavorable iliofemoral anatomy or severe peripheral arterial disease (PAD). However, patients with aortic stenosis (AS) have a higher prevalence of for PAD because both diseases are consequences of atherosclerotic degenerative changes. Transsubclavian, transapical, and direct access to the ascending aorta by thoracotomy are alternative routes for the TAVI procedure. In this report, we present the first Korean patient with symptomatic severe AS and bilateral iliofemoral artery disease who was successfully treated with TAVI using a CoreValve (Medtronic, Minneapolis, MN, USA) by transsubclavian approach.
MeSH Terms
Figure
-
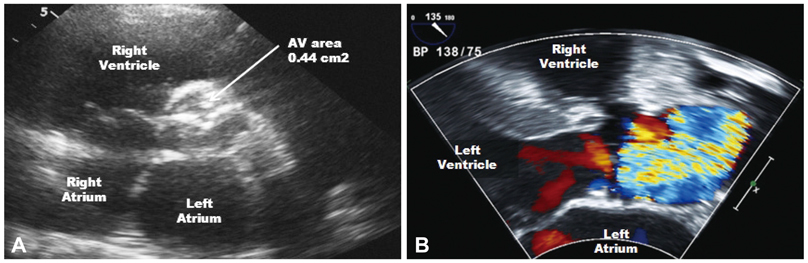
Fig. 1 Transthoracic echocardiography showed severely narrowed aortic valve area (0.44 cm2) measured by the continuity equation (A), and color Doppler revealed aliasing due to severe aortic stenosis (B).
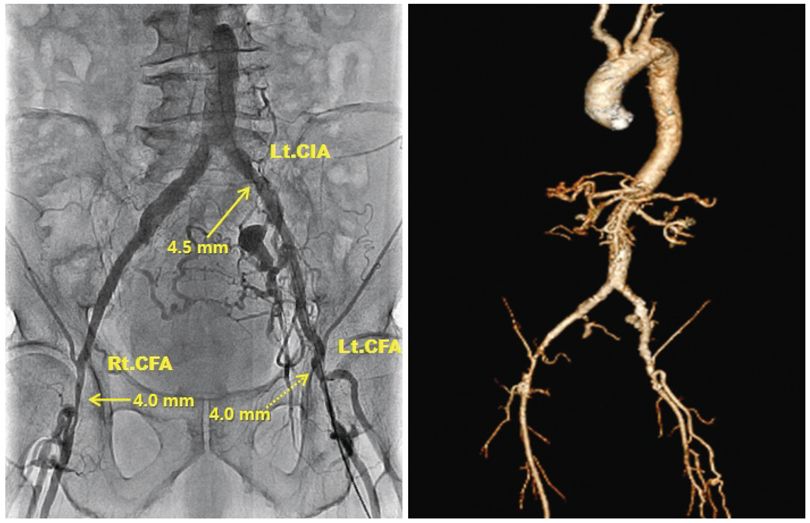
Fig. 2 Angiography and computed tomography image showed iliofemoral arteries with severe peripheral arterial occlusive disease. Previous stent at Lt. common iliac artery was patent but showed a minimum diameter of 4.5 mm and both common femoral arteries showed a minimum diameter of 4.0 mm. Lt. CIA: left common iliac artery, Rt. CFA: right common femoral artery, Lt. CFA: left common femoral artery.

Fig. 3 CoreValve delivery system is advanced through 18 Fr sheath inserted into the Lt. subclavian artery.
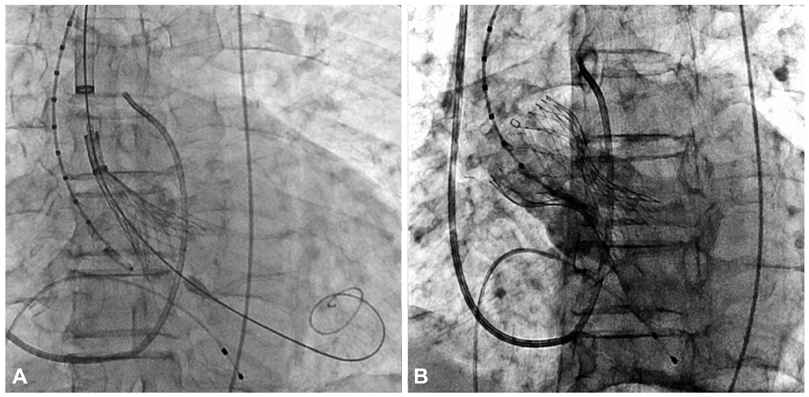
Fig. 4 CoreValve delivery catheter and bioprosthetic valve deployed across the aortic valve (A) and spontaneously expanded. An aortogram showed good positioning of the CoreValve with mild aortic regurgitation (B).
Reference
-
1. Iung B, Cachier A, Baron G, et al. Decision-making in elderly patients with severe aortic stenosis: why are so many denied surgery? Eur Heart J. 2005. 26:2714–2720.2. Aronow WS, Ahn C, Kronzon I. Association of valvular aortic stenosis with symptomatic peripheral arterial disease in older persons. Am J Cardiol. 2001. 88:1046–1047.3. Bruschi G, De Marco F, Fratto P, et al. Direct aortic access through right minithoracotomy for implantation of self-expanding aortic bioprosthetic valves. J Thorac Cardiovasc Surg. 2010. 140:715–717.4. Da Gama Ribeiro V, Vouga L, Markowitz A, et al. Vascular access in transcatheter aortic valve implantation. Int J Cardiovasc Imaging. 2011. 27:1235–1243.5. Bosmans JM, Kefer J, De Bruyne B, et al. Procedural, 30-day and one year outcome following CoreValve or Edwards transcatheter aortic valve implantation: results of the Belgian National Registry. Interact Cardiovasc Thorac Surg. 2011. 12:762–767.6. Witkowski A, Dąbrowski M, Chmielak Z, et al. Transcatheter aortic valve implantation using transfemoral/transsubclavian or transapical approach: 30-day follow-up of the initial 30 patients. Kardiol Pol. 2011. 69:105–114.7. Petronio AS, De Carlo M, Bedogni F, et al. Safety and efficacy of the subclavian approach for transcatheter aortic valve implantation with the CoreValve revalving system. Circ Cardiovasc Interv. 2010. 3:359–366.8. Moynagh AM, Scott DJ, Baumbach A, et al. CoreValve transcatheter aortic valve implantation via the subclavian artery: comparison with the transfemoral approach. J Am Coll Cardiol. 2011. 57:634–635.9. Fraccaro C, Napodano M, Tarantini G, et al. Expanding the eligibility for transcatheter aortic valve implantation the trans-subclavian retrograde approach using: the III generation CoreValve revalving system. JACC Cardiovasc Interv. 2009. 2:828–833.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transcatheter Aortic Valve Implantation by Transfemoral Approach in a Patient with Bilateral Iliac Artery Disease
- A Case of Severe Aortic Stenosis Patient With High Operative Risk Treated by Transcatheter Aortic-Valve Implantation
- Similar Morphology, but Different Function: Acute Improvement of Myocardial Longitudinal Strain after Percutaneous Transcatheter Aortic Valve Implantation Therapy in a Severe Aortic Stenosis Patient
- Expanding transcatheter aortic valve replacement into uncharted indications
- Anesthetic considerations of percutaneous transcatheter aortic valve implantation: first attempt in Korea: A report of 2 cases
