Pediatric Tachyarrhythmia and Radiofrequency Catheter Ablation: Results From 1993 to 2011
- Affiliations
-
- 1Department of Pediatrics, Keimyung University Dongsan Medical Center, Daegu, Korea. kimyhped@hanmail.net
- 2Division of Cardiology, Department of Internal Medicine, Keimyung University Dongsan Medical Center, Daegu, Korea.
- 3Department of Pediatrics, Kyungpook National University Hospital, Daegu, Korea.
- KMID: 2224972
- DOI: http://doi.org/10.4070/kcj.2012.42.11.735
Abstract
- BACKGROUND AND OBJECTIVES
We performed a retrospective study to elucidate the frequency of tachycardia mechanisms and the characteristics of accessory pathways (APs), confirmed by radiofrequency catheter ablation (RFCA) in pediatric tachycardia. In addition, we analyzed the efficacy and safety of pediatric RFCA.
SUBJECTS AND METHODS
The authors retrospectively reviewed the records of a total of 260 patients (aged 2 to 18 years) who had undergone RFCA between August 1993 and July 2011 at two medical centers in Daegu.
RESULTS
Two hundred and sixty patients underwent 272 RFCAs at less than 18 years of age. Of these 260 patients, 9 patients (3%) were younger than 6 years, and 175 patients (67%) were older than 12 years. The tachycardia mechanisms observed were atrioventricular reentry tachycardia (AVRT) in 175 patients (65%), atrioventricular nodal reentry tachycardia (AVNRT) in 83 patients (30%), ventricular tachycardia in 12 patients (4%), and atrial tachycardia in 2 patients (0.7%). Among the patients with AVRT, there were 94 concealed APs and 81 manifest APs. Left-side APs were more common in concealed APs than in manifest APs (72/94, 77% vs. 33/81, 41%, p<0.001). Sixty-six percent (55/83) of AVNRT cases were located at the M1 and/or M2 sites. Four patients had multiple tachycardia mechanisms (AVNRT+AVRT) and 9 patients had multiple APs. The recurrence rate was 5% (13/272). Of these recurrent cases, 12 patients had AVRT. The overall success rate was 95%.
CONCLUSION
Pediatric RFCA provides a good success rate and an acceptable recurrence. In addition, we suggest that the APs location may be associated with concealed or manifest property of APs.
MeSH Terms
Figure
-
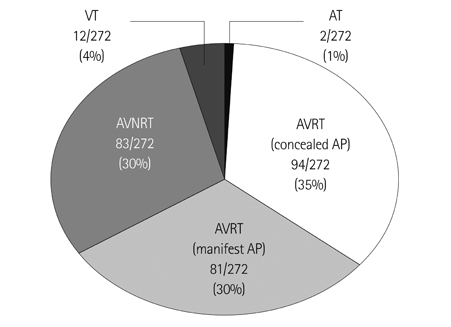
Fig. 1 The classification according to tachycardia mechanism. The most common tachycardia mechanism was AVRT. AVRT occurred more frequently than AVNRT (65% vs. 30%, p=0.0001). AVRT: atrioventricular reentry tachycardia, AVNRT: atrioventricular nodal reentry tachycardia, VT: ventricular tachycardia, AT: atrial tachycardia, AP: accessory pathway.
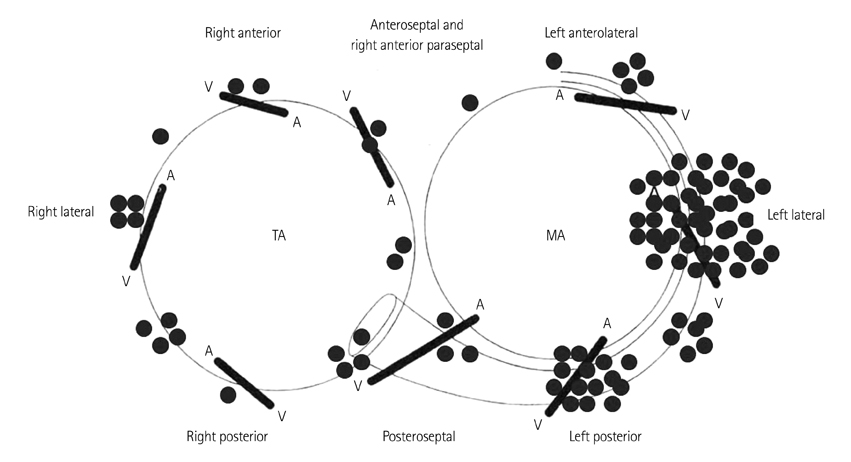
Fig. 2 The locations of APs in atrioventricular reentry tachycardia induced by concealed APs. In 94 patients, 79% of APs (74/94) was located on the left. The most common site for left-side APs was the left lateral wall (43/74, 58%). APs: accessory pathways, TA: tricuspid annulus, MA: mitral annulus.
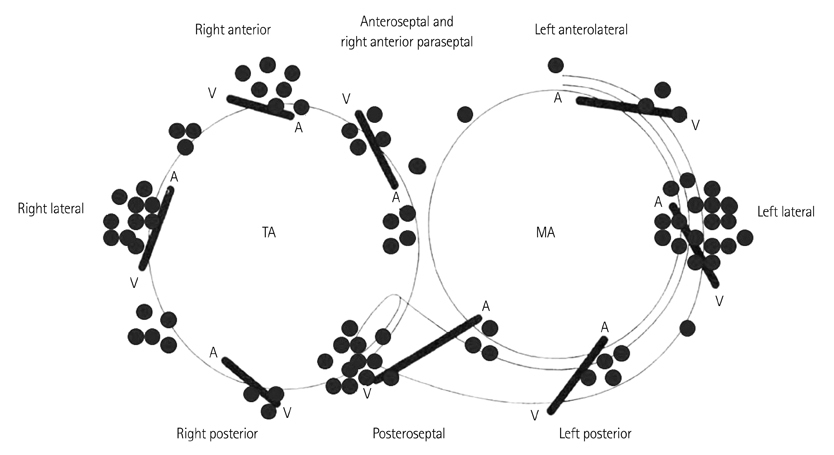
Fig. 3 locations of APs in atrioventricular reentry tachycardia with manifest APs. In 81 patients, 60% of APs (49/81) was located on the right. The three most common sites of AP were the left lateral wall (19/81, 23%), the right posteroseptal wall (12/81, 15%), and the right lateral wall (10/81, 12%). APs: accessory pathways, TA: tricuspid annulus, MA: mitral annulus.
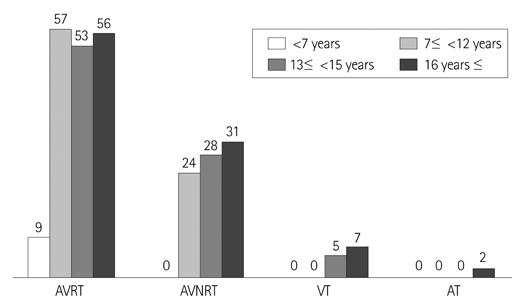
Fig. 4 Age related changes in tachycardia mechanisms. The most frequent tachycardia mechanism was AVRT. Although AVNRT occurred more common in older age than in younger age, there was no significant difference between tachycardia mechanism and age. AVRT: atrioventricular reentry tachycardia, AVNRT: atrioventricular nodal reentry tachycardia, VT: ventricular tachycardia, AT: atrial tachycardia.
Reference
-
1. Van Hare GF, Lesh MD, Scheinman M, Langberg JJ. Percutaneous radiofrequency catheter ablation for supraventricular arrhythmias in children. J Am Coll Cardiol. 1991. 17:1613–1620.2. Dick M 2nd, O'Connor BK, Serwer GA, LeRoy S, Armstrong B. Use of radiofrequency current to ablate accessory connections in children. Circulation. 1991. 84:2318–2324.3. Wu MH, Lin JL, Lai LP, et al. Radiofrequency catheter ablation of tachycardia in children with and without congenital heart disease: indications and limitations. Int J Cardiol. 2000. 72:221–227.4. Joung B, Lee M, Sung JH, Kim JY, Ahn S, Kim S. Pediatric radiofrequency catheter ablation: sedation methods and success, complication and recurrence rates. Circ J. 2006. 70:278–284.5. Bae EJ, Ban JE, Lee JA, et al. Pediatric radiofrequency catheter ablation: results of initial 100 consecutive cases including congenital heart anomalies. J Korean Med Sci. 2005. 20:740–746.6. Friedman RA, Walsh EP, Silka MJ, et al. North American Society of Pacing and Electrophysiology. NASPE Expert Consensus Conference: radiofrequency catheter ablation in children with and without congenital heart disease. Report of the writing committee. Pacing Clin Electrophysiol. 2002. 25:1000–1017.7. Akhtar M, Jazayeri MR, Sra J, Blanck Z, Deshpande S, Dhala A. Atrioventricular nodal reentry. Clinical, electrophysiological, and therapeutic considerations. Circulation. 1993. 88:282–295.8. Silka MJ, Kron J, Halperin BD, McAnulty JH. Mechanisms of AV node reentrant tachycardia in young patients with and without dual AV node physiology. Pacing Clin Electrophysiol. 1994. 17(11 Pt 2):2129–2133.9. Orejarena LA, Vidaillet H Jr, DeStefano F, et al. Paroxysmal supraventricular tachycardia in the general population. J Am Coll Cardiol. 1998. 31:150–157.10. Ko JK, Deal BJ, Strasburger JF, Benson DW Jr. Supraventricular tachycardia mechanisms and their age distribution in pediatric patients. Am J Cardiol. 1992. 69:1028–1032.11. Ludomirsky A, Garson A Jr. Gillette P, Garson A, editors. Supraventricular tachycardia. Pediatric Arrhythmias: Electrophysiology and Pacing. 1990. Philadelphia: W.B. Saunders Company;380–426.12. Blaufox AD, Rhodes JF, Fishberger SB. Age related changes in dual AV nodal physiology. Pacing Clin Electrophysiol. 2000. 23(4 Pt 1):477–480.13. Cohen MI, Wieand TS, Rhodes LA, Vetter VL. Electrophysiologic properties of the atrioventricular node in pediatric patients. J Am Coll Cardiol. 1997. 29:403–407.14. Silka MJ, Halperin BD, Hardy BG, McAnulty JH, Kron J. Safety and efficacy of radiofrequency modification of slow pathway conduction in children < or = 10 years of age with atrioventricular node reentrant tachycardia. Am J Cardiol. 1997. 80:1364–1367.15. Waki K, Kim JS, Becker AE. Morphology of the human atrioventricular node is age dependent: a feature of potential clinical significance. J Cardiovasc Electrophysiol. 2000. 11:1144–1151.16. Jung HJ, Ju HY, Hyun MC, Lee SB, Kim YH. Wolff-Parkinson-White syndrome in young people, from childhood to young adulthood: relationships between age and clinical and electrophysiological findings. Korean J Pediatr. 2011. 54:507–511.17. Lee PC, Hwang B, Chen YJ, Tai CT, Chen SA, Chiang CE. Electrophysiologic characteristics and radiofrequency catheter ablation in children with Wolff-Parkinson-White syndrome. Pacing Clin Electrophysiol. 2006. 29:490–495.18. Brembilla-Perrot B, Yangni N'da O, Huttin O, et al. Wolff-Parkinson-White syndrome in the elderly: clinical and electrophysiological findings. Arch Cardiovasc Dis. 2008. 101:18–22.19. Chiu SN, Lu CW, Chang CW, et al. Radiofrequency catheter ablation of supraventricular tachycardia in infants and toddlers. Circ J. 2009. 73:1717–1721.20. Van Hare GF, Chiesa NA, Campbell RM, Kanter RJ, Cecchin F. Pediatric Electrophysiology Society. Atrioventricular nodal reentrant tachycardia in children: effect of slow pathway ablation on fast pathway function. J Cardiovasc Electrophysiol. 2002. 13:203–209.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful Treatment of Tachycardia-induced Cardiomyopathy with Radiofrequency Catheter Ablation
- A Case of Chronic Radiodermatitis following Radiofrequency Catheter Ablation for Atrial Fibrillation
- Catheter ablation for treatment of tachyarrhythmia
- Conservative Management of Left Atrial Intramural Hematoma after Catheter Ablation
- Successful Management of Atrio-Esophageal Fistula after Cardiac Radiofrequency Catheter Ablation
