A Rare Combination of the Left Circumflex Coronary Artery Fistula Connecting a Dilated Coronary Sinus with Persistent Left Superior Vena Cava and Multiple Arteriovenous Fistulae
- Affiliations
-
- 1Cardiovascular Center of Chungbuk National University Hospital, Cheongju, Korea. sangmin3410@gmail.com
- KMID: 2224938
- DOI: http://doi.org/10.4070/kcj.2013.43.5.356
Abstract
- Coronary artery fistula (CAF) is an abnormal communication between an epicardial coronary artery and a cardiac chamber, major vessel or other vascular structures. This report presents a rare case of CAF in which a dilated left main trunk and proximal circumflex coronary artery are connected to a dilated coronary sinus. There were also two other fistulae and persistent left superior vena cava. The coronary fistula was managed conservatively.
MeSH Terms
Figure
-

Fig. 1 Echocardiographic findings. A: echocardiography shows a dilated coronary sinus. B: echocardiography shows a dilated left main coronary artery and abnormal color flow at the pulmonary valve level. Arrow indicating left main trunk and turbulent flow. LV: left ventricle, CS: coronary sinus, LA: left atrium, Ao: aorta.
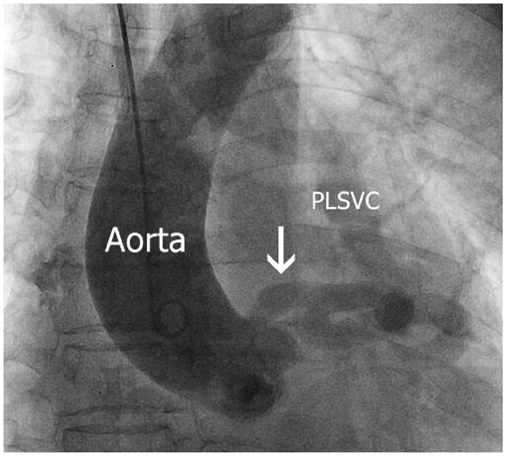
Fig. 2 Coronary angiography. Coronary angiography showing aneurysmal tortuous dilation of circumflex coronary artery and PLSVC. Arrow indicating dilated left main coronary artery. The exact drainage site of coronary artery fistula is not clearly identified. PLSVC: persistent left superior vena cava.
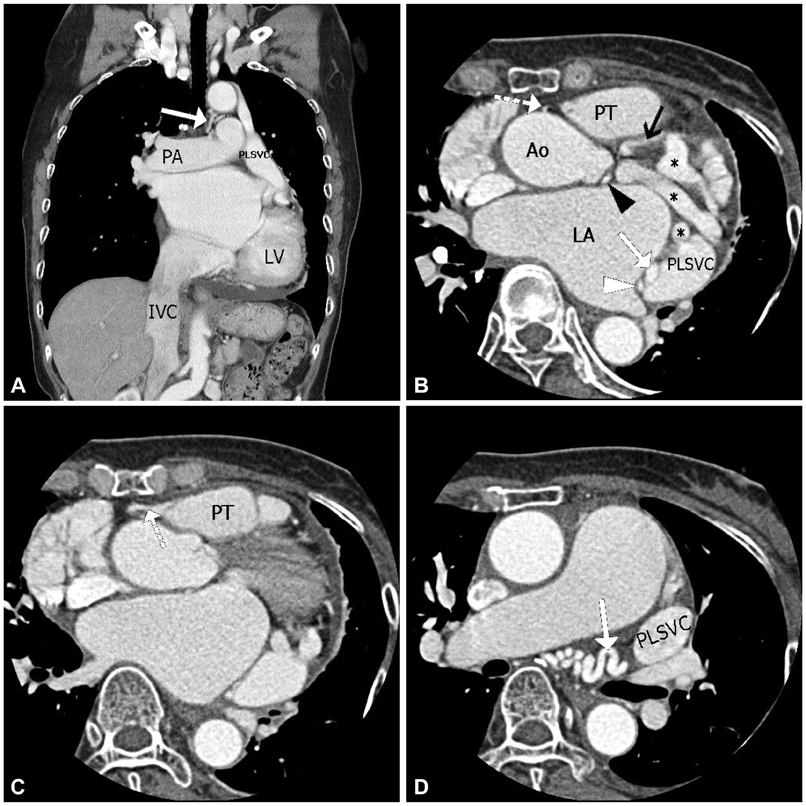
Fig. 3 A computed tomogram angiography. A: a coronal image from CT angiogram showing PLSVC. White arrow indicating the left bronchial artery, which originates from the descending aorta. B: an axial image from CT angiogram showing the left anterior descending coronary artery (black arrow), the tortuous fistula originating from the left circumflex coronary artery (*), the fistula originating from the sinoatrial nodal artery (white arrowhead), the fistula arising from the RCA and draining into the PT (white dotted arrow), termination of the left bronchial artery (white arrow). C: the white dotted arrow indicate conal branch originating from the RCA draining into the PT. D: an axial image from CT angiogram showing extremely tortuous left bronchial artery originate from the descending aorta (white dotted arrow). PLSVC: persistent left superior vena cava, LV: left ventricle, PA: pulmonary artery, IVC: inferior vena cava, PT: pulmonary trunk, Ao: aorta, LV: left ventricle, RCA: right coronary artery.
Reference
-
1. Makaryus AN, Stechel R, Green S. A rare combination of LMCA fistula to left superior vena cava with drainage into the coronary sinus in a 74-year-old woman. J Invasive Cardiol. 2003; 15:270–272.2. Chowdhury UK, Rizhvi A, Sheil A, et al. Successful surgical correction of a patient with congenital coronary arteriovenous fistula between left main coronary artery and right superior cavo-atrial junction. Hellenic J Cardiol. 2009; 50:73–78.3. Early SA, Meany TB, Fenlon HM, Hurley J. Coronary artery fistula; coronary computed topography--the diagnostic modality of choice. J Cardiothorac Surg. 2008; 3:41.4. Gufler H, Voigtlander T, Nowak B, Magedanz A, Schmermund A. Left circumflex coronary artery fistula to the superior vena cava: assessment of the exact anatomy by multidetector CT. Clin Res Cardiol. 2008; 97:272–276.5. Raju MG, Goyal SK, Punnam SR, Shah DO, Smith GF, Abela GS. Coronary artery fistula: a case series with review of the literature. J Cardiol. 2009; 53:467–472.6. Darwazah AK, Eida M, Batrawy M, Isleem I, Hanbali N. Surgical treatment of circumflex coronary aneurysm with fistulous connection to coronary sinus associated with persistent left superior vena cava. J Card Surg. 2011; 26:608–612.7. Abusaid GH, Hughes D, Khalife WI, Parto P, Gilani SA, Fujise K. Congenital coronary artery fistula presenting later in life. J Cardiol Cases. 2011; 4:e43–e46.8. Gandy KL, Rebeiz AG, Wang A, Jaggers JJ. Left main coronary artery-to-pulmonary artery fistula with severe aneurysmal dilatation. Ann Thorac Surg. 2004; 77:1081–1083.9. Abe T, Kamata K, Nakanishi K, Morishita K, Komatsu S. Successful repair of coronary artery-coronary sinus fistula with aneurysm in an adult. Ann Thorac Surg. 1996; 61:1520–1523.10. Zuberbuhler JR, Dankner E, Zoltun R, Burkholder J, Bahnson HT. Tissue adhesive closure of aortic-pulmonary communications. Am Heart J. 1974; 88:41–46.11. Ata Y, Turk T, Bicer M, Yalcin M, Ata F, Yavuz S. Coronary arteriovenous fistulas in the adults: natural history and management strategies. J Cardiothorac Surg. 2009; 4:62.12. Zhu XY, Zhang DZ, Han XM, et al. Transcatheter closure of congenital coronary artery fistulae: immediate and long-term follow-up results. Clin Cardiol. 2009; 32:506–512.13. Armsby LR, Keane JF, Sherwood MC, Forbess JM, Perry SB, Lock JE. Management of coronary artery fistulae. Patient selection and results of transcatheter closure. J Am Coll Cardiol. 2002; 39:1026–1032.14. Said SA. Congenital solitary coronary artery fistulas characterized by their drainage sites. World J Cardiol. 2010; 2:6–12.15. Kabbani Z, Garcia-Nielsen L, Lozano ML, Febles T, Febles-Bethencourt L, Castro A. Coil embolization of coronary artery fistulas. A single-centre experience. Cardiovasc Revasc Med. 2008; 9:14–17.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Congenital Giant Right Coronary Artery Aneurysm With Fistula to the Coronary Sinus and Persistent Left Superior Vena Cava in an Old Woman
- Giant Coronary Sinus Caused by Absent Right and Persistent Left Superior Vena Cava and Severe Tricuspid Regurgitation
- A Case of Persistent Left SVC Associated with Tricuspid Regurgitation
- A Case of Bilateral Long Coronary Arteriovenous Fistula
- Unroofed Coronary Sinus Associated with Persistent Left Superior Vena Cava : Detection by Agitated Saline Contrast Echocardiography
