Electrophysiological Characteristics Related to Outcome after Catheter Ablation of Idiopathic Ventricular Arrhythmia Originating from the Papillary Muscle in the Left Ventricle
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Korea University Medical Center, Seoul, Korea. yhkmd@unitel.co.kr
- 2Division of Cardiology, Department of Internal Medicine, Hanyang University Guri Hospital, Guri, Korea.
- KMID: 2224775
- DOI: http://doi.org/10.4070/kcj.2013.43.12.811
Abstract
- BACKGROUND AND OBJECTIVES
The electrophysiological properties associated with favorable outcome of radiofrequency catheter ablation (RFCA) for idiopathic ventricular arrhythmia (VA) originating from the papillary muscle (PM) remain unclear. The purpose of this study was to investigate the relationships of electrophysiological characteristics and predictors with the outcome of RFCA in patients with VAs originating from PM in the left ventricle (LV).
SUBJECTS AND METHODS
Twelve (4.2%) of 284 consecutive patients with idiopathic VAs originating from LV PM were assessed. The electrophysiological data were compared between the patients in the successful group and patients in the recurrence group after RFCA.
RESULTS
In 12 patients with PM VAs, non-sustained ventricular tachycardias (VTs, n=6), sustained VTs (n=4) and premature ventricular complexes (n=2) were identified as the presenting arrhythmias. Seven of eight patients showing high-amplitude discrete potentials at the ablation site had a successful outcome (85.7%), while the remaining four patients who showed low-amplitude fractionated potentials at the ablation site experienced VA recurrence. The mean duration from onset to peak downstroke (Deltat) on the unipolar electrogram was significantly longer in the successful group than in the recurrence group (58+/-8 ms vs. 37+/-9 ms, p=0.04). A slow downstroke >50 ms of the initial Q wave on the unipolar electrogram at ablation sites was also significantly associated with successful outcome (85.7% vs. 25.0%, p=0.03).
CONCLUSION
In PM VAs, the high-amplitude discrete potentials before QRS and slow downstroke of the initial Q wave on the unipolar electrogram at ablation sites were related to favorable outcome after RFCA.
MeSH Terms
Figure
-

Fig. 1 The 12-lead ECG of ventricular arrhythmias originating from the posterior papillary muscle in the left ventricle. A: the representative 12-lead ECG of a non-sustained VT originating from the LV PPM. B: notches in precordial leads during VAs originating from the LV PPM (left panel) and LV APM (right panel). Arrows indicate notches in the precordial leads. ECG: electrocardiogram, VT: ventricular tachycardia, LV: left ventricle, PPM: posterior papillary muscle, VAs: ventricular arrhythmias, APM: anterior papillary muscle.
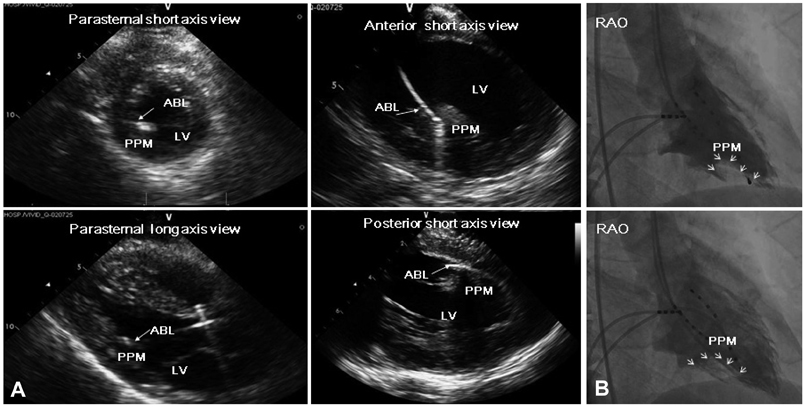
Fig. 2 The echocardiographic and fluoroscopic images exhibiting the successful ablation site. A: the echocardiographic image of the successful ablation site. A two-dimensional transthoracic echocardiographic (left panel) and intra-cardiac echocardiographic (right panel) image at the level of the PM demonstrated that the ablation catheter was positioned on the base of the PPM. Transthoracic echocardiography showed the exact ablation catheter laid at the PPM in the parasternal short axis and long axis view, respectively (left panel). The anterior and posterior short axis view intra-cardiac echocardiography showed the ablation catheter on the base of PPM in the LV (right panel). The arrow indicates the ablation catheter. B: right anterior oblique fluoroscopic image of the successful ablation site referenced to left ventriculograms. The small arrows indicate the border of the PPM during left ventricular systole (upper panel) and diastole (lower panel). ABL: ablation catheter, LV: left ventricle, PM: papillary muscle, PPM: posterior papillary muscle, RAO: right anterior oblique view.

Fig. 3 Local bipolar electrogram, unipolar electrogram and three-dimensional electroanatomic mapping images of successful (A) and unsuccessful (B) ablation sites of VT originating from the PPM in the LV. A: a high-amplitude discrete potential (arrow) from the distal bipole of the ablation catheter was recorded during VT (left panel) and Purkinje potential (asterisk) during sinus rhythm (middle panel) at the site of successful ablation. A relatively slow downstroke of initial Q wave on unipolar electrogram was observed. The duration from onset to peak downstroke was 62 ms. The three-dimensional electroanatomical mapping (right panel) obtained during procedure in the right and left anterior oblique view showed the color-coded voltage map (right upper panel) and successful ablation site (right lower panel) of the PPM in the LV. White dots represent the site of RFCA. White arrows indicate the PPM area in the LV. B: a low-amplitude myocardial potential (arrow) recorded during VT from the distal bipole of the ablation catheter preceded the onset of QRS by 34 ms. A relatively steep downstroke of initial Q wave on unipolar electrogram was observed at the unsuccessful ablation site (left panel). The duration from onset to peak downstroke was 42 ms. No Purkinje potential was shown during sinus rhythm (right panel). ABL: ablation catheter, LAO: left anterior oblique view, LV: left ventricle, PPM: posterior papillary muscle, RAO: right anterior oblique view, RVA: right ventricular apex, SR: sinus rhythm, VT: ventricular tachycardia, RFCA: radiofrequency catheter ablation, Δt: the time from the initial QS wave onset to the initial QS wave peak on unipolar electrogram.
Reference
-
1. Kim YH, Xie F, Yashima M, et al. Role of papillary muscle in the generation and maintenance of reentry during ventricular tachycardia and fibrillation in isolated swine right ventricle. Circulation. 1999; 100:1450–1459.2. Pak HN, Kim YH, Lim HE, et al. Role of the posterior papillary muscle and purkinje potentials in the mechanism of ventricular fibrillation in open chest dogs and Swine: effects of catheter ablation. J Cardiovasc Electrophysiol. 2006; 17:777–783.3. Chen PS, Karagueuzian HS, Kim YH. Papillary muscle hypothesis of idiopathic left ventricular tachycardia. J Am Coll Cardiol. 2001; 37:1475–1476.4. Yamada T, Tabereaux PB, Doppalapudi H, McElderry HT, Kay GN. Successful catheter ablation of a ventricular tachycardia storm originating from the left ventricular posterior papillary muscle involved with a remote myocardial infarction. J Interv Card Electrophysiol. 2009; 24:143–145.5. Liu XK, Barrett R, Packer DL, Asirvatham SJ. Successful management of recurrent ventricular tachycardia by electrical isolation of anterolateral papillary muscle. Heart Rhythm. 2008; 5:479–482.6. Bogun F, Desjardins B, Crawford T, et al. Post-infarction ventricular arrhythmias originating in papillary muscles. J Am Coll Cardiol. 2008; 51:1794–1802.7. Doppalapudi H, Yamada T, McElderry HT, Plumb VJ, Epstein AE, Kay GN. Ventricular tachycardia originating from the posterior papillary muscle in the left ventricle: a distinct clinical syndrome. Circ Arrhythm Electrophysiol. 2008; 1:23–29.8. Good E, Desjardins B, Jongnarangsin K, et al. Ventricular arrhythmias originating from a papillary muscle in patients without prior infarction: a comparison with fascicular arrhythmias. Heart Rhythm. 2008; 5:1530–1537.9. Yamada T, McElderry HT, Okada T, et al. Idiopathic focal ventricular arrhythmias originating from the anterior papillary muscle in the left ventricle. J Cardiovasc Electrophysiol. 2009; 20:866–872.10. Yamada T, Doppalapudi H, McElderry HT, et al. Idiopathic ventricular arrhythmias originating from the papillary muscles in the left ventricle: prevalence, electrocardiographic and electrophysiological characteristics, and results of the radiofrequency catheter ablation. J Cardiovasc Electrophysiol. 2010; 21:62–69.11. Yamada T, Doppalapudi H, McElderry HT, et al. Electrocardiographic and electrophysiological characteristics in idiopathic ventricular arrhythmias originating from the papillary muscles in the left ventricle: relevance for catheter ablation. Circ Arrhythm Electrophysiol. 2010; 3:324–331.12. Crawford T, Mueller G, Good E, et al. Ventricular arrhythmias originating from papillary muscles in the right ventricle. Heart Rhythm. 2010; 7:725–730.13. Yokokawa M, Good E, Desjardins B, et al. Predictors of successful catheter ablation of ventricular arrhythmias arising from the papillary muscles. Heart Rhythm. 2010; 7:1654–1659.14. Nogami A, Naito S, Tada H, et al. Demonstration of diastolic and presystolic Purkinje potentials as critical potentials in a macroreentry circuit of verapamil-sensitive idiopathic left ventricular tachycardia. J Am Coll Cardiol. 2000; 36:811–823.15. Aiba T, Suyama K, Aihara N, et al. The role of Purkinje and pre-Purkinje potentials in the reentrant circuit of verapamil-sensitive idiopathic LV tachycardia. Pacing Clin Electrophysiol. 2001; 24:333–344.16. Maruyama M, Tadera T, Miyamoto S, Ino T. Demonstration of the reentrant circuit of verapamil-sensitive idiopathic left ventricular tachycardia: direct evidence for macroreentry as the underlying mechanism. J Cardiovasc Electrophysiol. 2001; 12:968–972.17. Zipes DP. Mechanisms of clinical arrhythmias. J Cardiovasc Electrophysiol. 2003; 14:902–912.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiofrequency Ablation of Recurrent Ventricular Premature Complex Originating from near Left Ventricular Summit Guided by Intracardiac Echocardiography
- Left atrial ıntramural hematoma after radiofrequency catheter ablation of left lateral accessory pathway
- Electroanatomical Characteristics of Idiopathic Left Ventricular Tachycardia and Optimal Ablation Target during Sinus Rhythm: Significance of Preferential Conduction through Purkinje Fibers
- Atrial Tachycardia Originating from the Aortomitral Junction
- Intramural Reentrant Ventricular Tachycardia in a Patient with Severe Hypertensive Left Ventricular Hypertrophy
