Atrial Tachycardia Originating from the Aortomitral Junction
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. cby6908@yuhs.ac
Abstract
- Atrial tachycardia (AT) originating from the aortomitral junction is a very rare and challenging disease. Its arrhythmic characteristics have not been described in detail compared with the descriptions of the arrhythmic characteristics of AT originating from the other locations. Only a few case reports have documented successful ablation of this type of AT using transaortic or transseptal approaches. We describe a case with AT that was resistant to right-sided ablation near the His bundle failed and transaortic ablation at the aortomitral junction successfully eliminated.
MeSH Terms
Figure
-

Fig. 1 Surface 12-lead electrocardiogram during an episode of palpitation, showing a narrow QRS complex tachycardia with a cycle length of 350 ms. The P-wave polarity preceding the QRS complex was isoelectric in lead I and biphasic in leads V1 and V3.
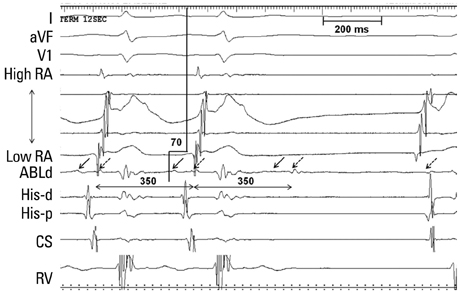
Fig. 2 Intracardiac electrograms and ablation signal at the earliest mapped location in the aortomitral junction. The earliest atrial activation (arrow) was found at the aortomitral junction, where the local electrogram recorded from the distal electrodes of the ablation catheter during tachycardia preceded the onset of the surface P wave by 70 ms. Note that the earliest atrial electrogram recorded from the distal ablation catheter (ABLd) also has a large ventricular potential. Tachycardia was terminated 12 s after radiofrequency application. RA, right atrium; CS, coronary sinus; RV, right ventricle.
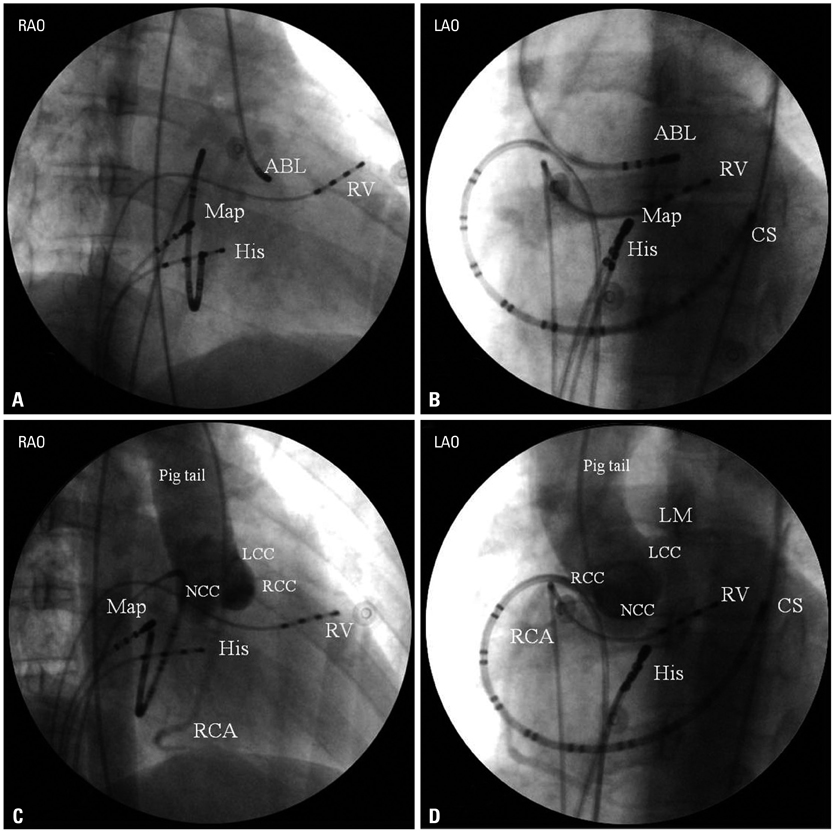
Fig. 3 Fluoroscopic images in orthogonal fluoroscopic view. (A and B) The successful catheter ablation (ABL) site in the right anterior oblique (RAO) and left anterior oblique (LAO) views, located in the aortomitral junction. (C and D) Aortic root angiograms taken from a pigtail catheter placed at the right coronary cusp (RCC), with the same fluoroscopic angles before ablation. In the RAO view, the RCC overlaps with the left coronary cusp (LCC), and the most anterior aspect is the junction of RCC/LCC. In this view, the NCC is located at the most posterior aspect of the aorta. In the LAO view, the RCC overlaps with the NCC, and the most rightward aspect is the junction of NCC/RCC. The LCC is located at the most leftward aspect in this view. Another mapping catheter (Map) in the RA positioned at the unsuccessful ablation site near the right His-bundle region. CS, coronary sinus; RV, right ventricle; NCC, non-coronary cusp.
Reference
-
1. Kay GN, Chong F, Epstein AE, Dailey SM, Plumb VJ. Radiofrequency ablation for treatment of primary atrial tachycardias. J Am Coll Cardiol. 1993; 21:901–909.
Article2. Chen SA, Chiang CE, Yang CJ, Cheng CC, Wu TJ, Wang SP, et al. Sustained atrial tachycardia in adult patients. Electrophysiological characteristics, pharmacological response, possible mechanisms, and effects of radiofrequency ablation. Circulation. 1994; 90:1262–1278.
Article3. Kalman JM, Olgin JE, Karch MR, Hamdan M, Lee RJ, Lesh MD. "Cristal tachycardias": origin of right atrial tachycardias from the crista terminalis identified by intracardiac echocardiography. J Am Coll Cardiol. 1998; 31:451–459.
Article4. Dong J, Schreieck J, Ndrepepa G, Schmitt C. Ectopic tachycardia originating from the superior vena cava. J Cardiovasc Electrophysiol. 2002; 13:620–624.
Article5. Morton JB, Sanders P, Das A, Vohra JK, Sparks PB, Kalman JM. Focal atrial tachycardia arising from the tricuspid annulus: electrophysiologic and electrocardiographic characteristics. J Cardiovasc Electrophysiol. 2001; 12:653–659.
Article6. Volkmer M, Antz M, Hebe J, Kuck KH. Focal atrial tachycardia originating from the musculature of the coronary sinus. J Cardiovasc Electrophysiol. 2002; 13:68–71.
Article7. Kistler PM, Sanders P, Fynn SP, Stevenson IH, Hussin A, Vohra JK, et al. Electrophysiological and electrocardiographic characteristics of focal atrial tachycardia originating from the pulmonary veins: acute and long-term outcomes of radiofrequency ablation. Circulation. 2003; 108:1968–1975.
Article8. Otomo K, Nagata Y, Uno K, Iesaka Y. "Left-variant" adenosine-sensitive atrial reentrant tachycardia ablated from the left coronary aortic sinus. Pacing Clin Electrophysiol. 2008; 31:247–250.
Article9. Shehata M, Liu T, Joshi N, Chugh SS, Wang X. Atrial tachycardia originating from the left coronary cusp near the aorto-mitral junction: anatomic considerations. Heart Rhythm. 2010; 7:987–991.
Article10. Wang Z, Liu T, Shehata M, Liang Y, Jin Z, Liang M, et al. Electrophysiological characteristics of focal atrial tachycardia surrounding the aortic coronary cusps. Circ Arrhythm Electrophysiol. 2011; 4:902–908.
Article11. Das S, Neuzil P, Albert CM, D'Avila A, Mansour M, Mela T, et al. Catheter ablation of peri-AV nodal atrial tachycardia from the noncoronary cusp of the aortic valve. J Cardiovasc Electrophysiol. 2008; 19:231–237.
Article12. Kriatselis C, Roser M, Min T, Evangelidis G, Höher M, Fleck E, et al. Ectopic atrial tachycardias with early activation at His site: radiofrequency ablation through a retrograde approach. Europace. 2008; 10:698–704.
Article13. Ouyang F, Ma J, Ho SY, Bänsch D, Schmidt B, Ernst S, et al. Focal atrial tachycardia originating from the non-coronary aortic sinus: electrophysiological characteristics and catheter ablation. J Am Coll Cardiol. 2006; 48:122–131.14. Wit AL, Cranefield PF. Triggered activity in cardiac muscle fibers of the simian mitral valve. Circ Res. 1976; 38:85–98.
Article15. Ho SY. Structure and anatomy of the aortic root. Eur J Echocardiogr. 2009; 10:i3–i10.
Article16. Marrouche NF, SippensGroenewegen A, Yang Y, Dibs S, Scheinman MM. Clinical and electrophysiologic characteristics of left septal atrial tachycardia. J Am Coll Cardiol. 2002; 40:1133–1139.
Article17. Markowitz SM, Nemirovksy D, Stein KM, Mittal S, Iwai S, Shah BK, et al. Adenosine-insensitive focal atrial tachycardia: evidence for de novo micro-re-entry in the human atrium. J Am Coll Cardiol. 2007; 49:1324–1333.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful Catheter Ablation of Atrial Tachycardia Originating from the Non-coronary Aortic Sinus
- Focal Atrial Tachycardia Arising from the Inferior Vena Cava
- Differential Diagnosis of Supraventricular Tachycardia
- Atrial Fibrillation with Ventricular Pre-excitation after Intravenous Adenosine as a Treatment of Supraventricular Tachycardia
- Spontaneous Transition of Double Tachycardias with Atrial Fusion in a Patient with Wolff-Parkinson-White Syndrome
