A Case of Development of Sarcoidosis During Tumor Necrosis Factor-alpha Antagonist Therapy
- Affiliations
-
- 1Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea.
- 2Department of Pathology, Hanyang University College of Medicine, Seoul, Korea.
- 3Department of Rheumatology, The Hospital for Rheumatic Diseases, Hanyang University College of Medicine, Seoul, Korea. thkim@hanyang.ac.kr
- KMID: 2223181
- DOI: http://doi.org/10.4078/jrd.2011.18.1.41
Abstract
- Etanercept is a soluble receptor fusion protein that inhibits tumor necrosis factor-alpha(TNF-alpha). The receptor is used widely in the treatment of ankylosing spondylitis, rheumatoid arthritis, sarcoidosis and other indications. For sarcoidosis, it potentially suppresses granuloma formation with TNF-alpha blocking. On the other hand, recent studies have suggested that paradoxical sarcoidosis can be induced by TNF-alpha antagonists in some cases. A 42-year-old woman, who was treated with etanercept due to ankylosing spondylitis for 5 years, was admitted because of right suprahilar lymphadenopathy on chest radiography. Chest computed tomography revealed an enlargement of supraclavicular, paratracheal, mediastinal lymph nodes. She was diagnosed with sarcoidosis on the supraclavicular lymph node biopsy, which was non-caseating epithelioid cell granuloma and excluded from similar diseases. She was treated for sarcoidosis with prednisolone instead of etanercept.
MeSH Terms
-
Adult
Arthritis, Rheumatoid
Biopsy
Epithelioid Cells
Female
Granuloma
Hand
Humans
Immunoglobulin G
Lymph Nodes
Lymphatic Diseases
Necrosis
Prednisolone
Receptors, Tumor Necrosis Factor
Sarcoidosis
Spondylitis, Ankylosing
Thorax
Tumor Necrosis Factor-alpha
Etanercept
Immunoglobulin G
Prednisolone
Receptors, Tumor Necrosis Factor
Tumor Necrosis Factor-alpha
Figure
-

Figure 1. Pelvis AP shows the erosive changes and focal subchondral sclerosis of the bilateral sacroiliac joints, which is com-patible with sacroiliitis, grade 3.
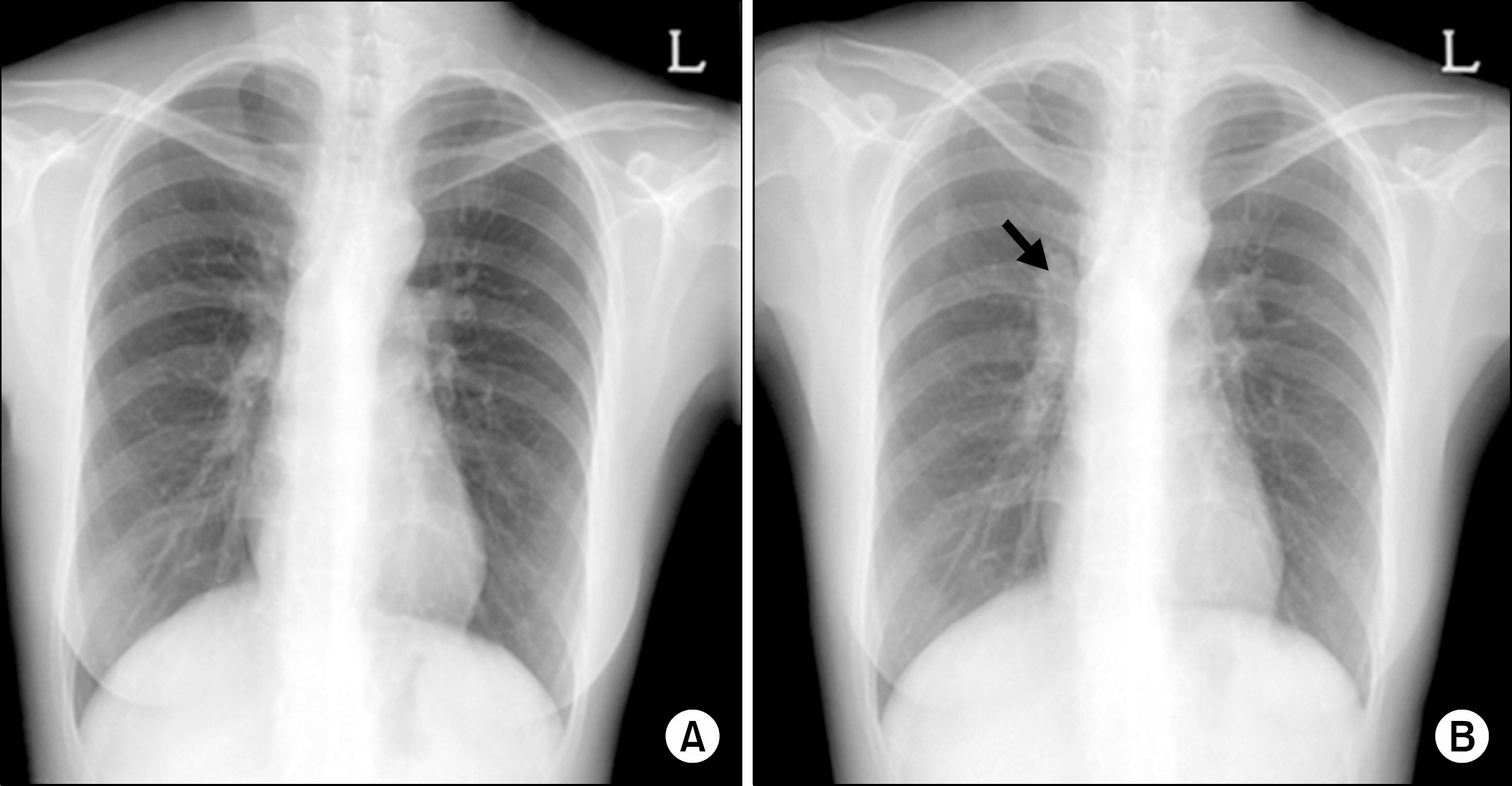
Figure 2. Chest PA shows normal findings 4 months earlier (A) and right suprahilar lymph node (arrow) enlargement at a regular followup (B).
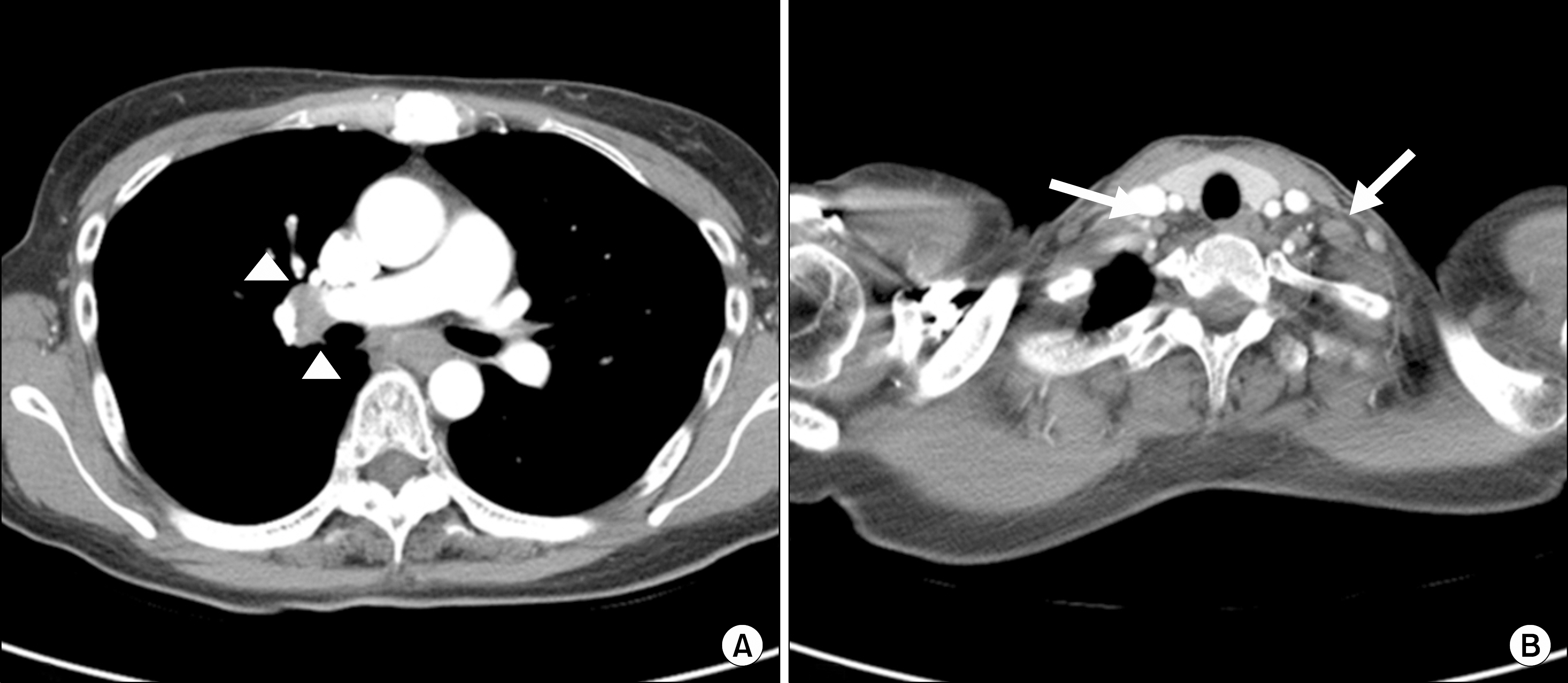
Figure 3. Chest CT scan showing right hilar, subcarinal lymphadenopathy (arrow head) (A) and left supraclavicular, right upper paratracheal lymphadenopathy (arrow) (B).
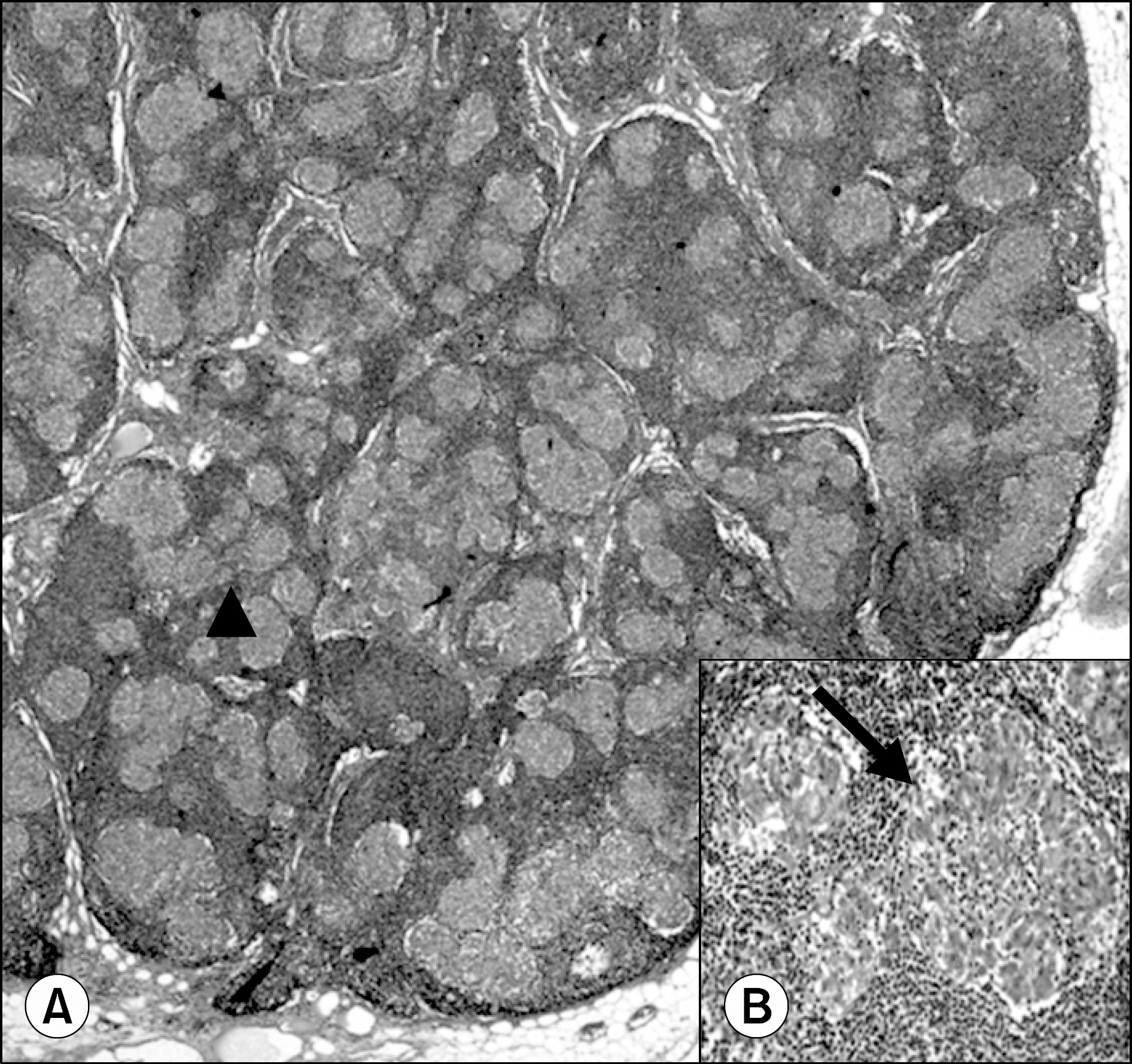
Figure 4. Supraclavicular lymph node biopsy showing evenly distributed small noncaseating granulomas (arrow) (A) (H&E stain, ×40) composed of epithelioid histiocytes (arrow) (B) (H&E stain, ×200).
Cited by 1 articles
-
A Case of Sarcoidosis That Improved upon Discontinuation of Etanercept
Ji-Hyoun Kang, Joon-Ho Ahn, Ji-Eun Yu, Ji-Eun Kim, Yi-Rang Yim, Jeong-Won Lee, Kyung-Eun Lee, Dong-Jin Park, Lihui Wen, Yong-Wook Park, Shin-Seok Lee
J Rheum Dis. 2016;23(3):187-192. doi: 10.4078/jrd.2016.23.3.187.
Reference
-
References
1. Baughman RP, Costabel U, du Bois RM. Treatment of sarcoidosis. Clin Chest Med. 2008; 29:533–48.2. Gonzá lez-López MA, Blanco R, González-Vela MC, Fernández-Llaca H, Rodríguez-Valverde V. Development of sarcoidosis during etanercept therapy. Arthritis Rheum. 2006; 55:817–20.3. Ishiguro T, Takayanagi N, Kurashima K, Matsushita A, Harasawa K, Yoneda K, et al. Development of sarcoidosis during etanercept therapy. Intern Med. 2008; 47:1021–5.4. Thomeer M, Demedts M, Wuyts W. Epidemiology of sarcoidosis. Eur Respir Mon. 2005; 32:13–22.5. Kim DS, Ahn JJ. Sacoidosis in Korea. Tuberc Respir Dis. 2000; 49:274–80.6. Gerke AK, Hunninghake G. The immunology of sarcoidosis. Clin Chest Med. 2008; 29:379–90.7. Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007; 357:2153–65.8. Ramos-Casals M, Roberto-Perez-Alvarez , Diaz-Lagares C, Cuadrado MJ, Khamashta MA. BIOGEAS Study Group. Autoimmune diseases induced by biological agents: a double-edged sword? Autoimmun Rev. 2010; 9:188–93.9. Furst DE, Wallis R, Broder M, Beenhouwer DO. Tumor necrosis factor antagonists: different kinetics and/or mechanisms of action may explain differences in the risk for developing granulomatous infection. Semin Arthritis Rheum. 2006; 36:159–67.10. Massara A, Cavazzini L, La Corte R, Trotta F. Sarcoidosis appearing during antitumor necrosis factor alpha therapy: a new "class effect" paradoxical phenomenon. Two case reports and literature review. Semin Arthritis Rheum. 2010; 39:313–9.11. Daïen CI, Monnier A, Claudepierre P, Constantin A, Eschard JP, Houvenagel E, et al. Club Rhumatismes et Inflammation (CRI). Sarcoid-like granulomatosis in patients treated with tumor necrosis factor blockers: 10 cases. Rheumatology (Oxford). 2009; 48:883–6.12. Dinarello CA. Differences between antitumor necrosis factor alpha monoclonal antibodies and soluble TNF receptors in host defense impairment. J Rheumatol Suppl. 2005; 74:40–7.13. van der Stoep D, Braunstahl GJ, van Zeben J, Wouters J. Sarcoidosis during antitumor necrosis factor-alpha therapy: no relapse after rechallenge. J Rheumatol. 2009; 36:2847–8.14. Choi BY, Park YB, Lee JH, Ryu HJ, Lee EY, Lee YJ, et al. A case of ankylosing spondylitis accompanying sarcoidosis. J Korean Rheum Assoc. 2007; 14:251–5.15. Stucki G, von Felten A, Speich R, Michel BA. Ankylosing spondylitis and sarcoidosis–coincidence or association? Case report and review of the literature. Clin Rheumatol. 1992; 11:436–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Ankylosing Spondylitis Accompanying Sarcoidosis
- A Case of Capecitabine-Induced Sarcoidosis
- A Case of Development of Vitiligo Followed by TNF-alpha Antagonist Treatment for Rheumatoid Arthritis
- A Case of Psoriasiform Eruption Triggered by Tumor Necrosis Factor-alpha Antagonist Therapy
- Tumor Necrosis Factor Alpha Blocker-Induced Erythrodermic Sarcoidosis in with Juvenile Rheumatoid Arthritis: A Case Report and Review of the Literature
