Acute Polymyositis/systemic Lupus Erythematosus Overlap Syndrome with Severe Subcutaneous Edema and Interstitial Lung Disease
- Affiliations
-
- 1Department of Rheumatology, Ajou University School of Medicine, Suwon, Korea. nakhada@ajou.ac.kr
- 2Department of Radiology, Ajou University School of Medicine, Suwon, Korea.
- 3Department of Pathology, Ajou University School of Medicine, Suwon, Korea.
- KMID: 2222985
- DOI: http://doi.org/10.4078/jrd.2014.21.1.25
Abstract
- Inflammatory myopathy is characterized by symmetrical proximal muscle weakness, elevated muscle enzyme levels and favorable response to glucocorticoids therapy. Although periorbital edema is a common manifestation of inflammatory myopathy, generalized subcutaneous edema is very rare. We report here a case of a 47-year-old female patient with acute polymyositis/systemic lupus erythematosus overlap syndrome with generalized subcutaneous edema and interstitial lung disease. We aggressively treated the disease with high-dose glucocorticoids, intravenous immunoglobulin, and immunosuppressive agents.
MeSH Terms
Figure
-

Figure 1. Gross appearance of generalized edema of upper (A) and lower extremities (B) in a 47-year-old woman with acute polymyositis.

Figure 2. Radiologic findings of computed tomography (CT) scan of the chest. (A) The CT scan of the chest upon admission shows interstitial lung disease with consolidation and ground-glass opacities in peripheral lungs, bilateral pleural effusion, and minimal pericardial effusion. (B) The resolution of the interstitial lung disease after treatment.
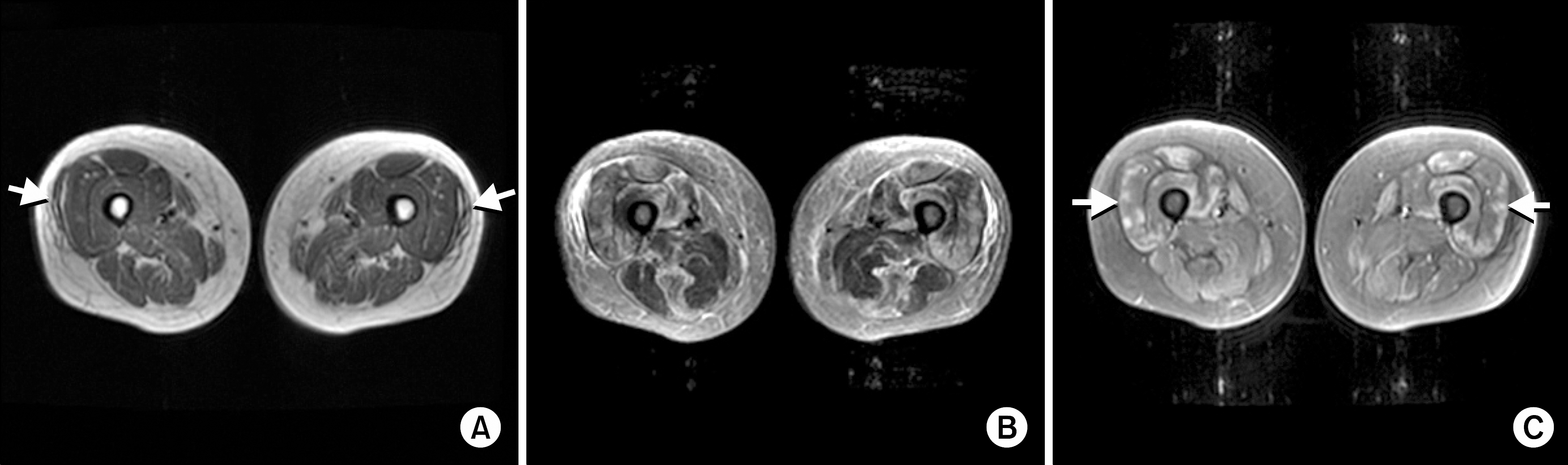
Figure 3. Radiologic findings of magnetic resonance imaging (MRI) of the thigh. (A) Axial T1-weighted image only shows generalized subcutaneous edema with focal low-signal subcutaneous fluid adjacent to vastus lateralis muscle (arrows). (B) Axial fat-suppressed fast spin-echo T2-weighted image shows a pattern of patchy elevated signal within multiple muscles in all three compartments. Biceps femoris, semimembranosus, and adductor magnus are relatively spared. (C) Axial fat-suppressed contrast-enhanced T1-weighted image shows a similar pattern of elevated signal within the affected muscles similar to the distribution seen on T2-weighted images. There is patchy enhancement of the quadriceps femoris group, sartorius, gracilis, and semitendinosus muscles (arrows).
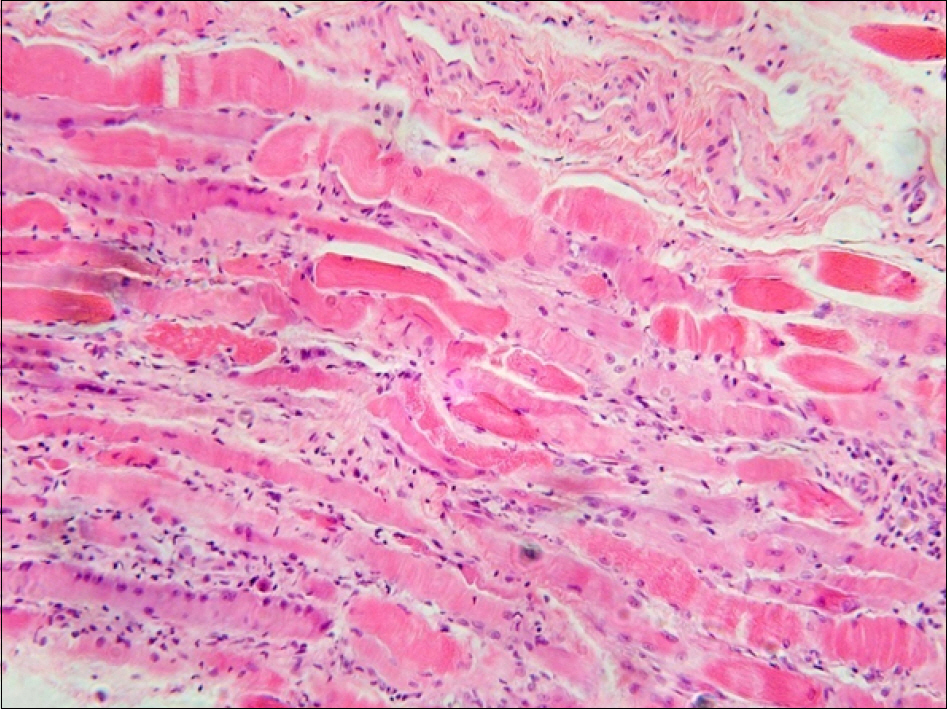
Figure 4. Biopsy specimen of left deltoid muscle revealing interstitial and perifascular inflammatory cell infiltrates, degenerating fibers, perivascular inflammatory cell infiltrates and interstitial fibrosis consistent with polymyositis (H&E, ×200).
Reference
-
References
1. Miller FW. New approaches to the assessment and treatment of the idiopathic inflammatory myopathies. Ann Rheum Dis. 2012; 71(Suppl 2):i82–5.
Article2. Dimachkie MM. Idiopathic inflammatory myopathies. J Neuroimmunol. 2011; 231:32–42.
Article3. Jung KD, Kim PS, Park HY, Kim CR, Byun JY, Lee DY, et al. Dermatomyositis associated with generalized subcutaneous edema and Evans syndrome. J Am Acad Dermatol. 2012; 66:144–7.
Article4. Lee KH, Lim SR, Kim YJ, Lee KJ, Myung DS, Jeong HC, et al. Acute dermatomyositis associated with generalized subcutaneous edema. Rheumatol Int. 2008; 28:797–800.
Article5. Werner de Castro GR, Appenzeller S, Bértolo MB, Costallat LT. Acute dermatomyositis with subcutaneous generalized edema. Clin Rheumatol. 2006; 25:898–900.
Article6. Mroué KH, Sharara NH, Rbeiz JG, Arayssi TK. A case of edematous dermatomyositis. J Rheumatol. 2003; 30:2722–3.7. Gorelik O, Almoznino-Sarafian D, Alon I, Rapoport MJ, Goltsman G, Herbert M, et al. Acute inflammatory myopathy with severe subcutaneous edema, a new variant? Report of two cases and review of the literature. Rheumatol Int. 2001; 20:163–6.8. Smyth AE, Bell AL, Crone M. Acute oedematous dermatomyositis. Ann Rheum Dis. 2000; 59:575.
Article9. Nitsche A, San Agustín PG, Amado V, Prina AP, Corsaro G. Trunk and abdominal wall edema in dermatomyositis. Medicina (B Aires). 1988; 48:331–2.10. Lyon-Caen O, Bouche P, Chaunu MP, Duyckaerts C, Vitoux JF. Acute polymyositis with spontaneously re-gressive subcutaneous edema. Apropos of a case. Rev Neurol (Paris). 1985; 141:749–52.11. Andonopoulos AP, Gogos CA, Tzanakakis G. Subcutaneous edema: an "unrecognized" feature of acute polymyositis. Rheumatol Int. 1993; 13:159–61.
Article12. Venables GS, Bates D, Cartlidge NE, Hudgson P. Acute polymyositis with subcutaneous oedema. J Neurol Sci. 1982; 55:161–4.
Article13. Haroon M, Eltahir A, Harney S. Generalized subcutaneous edema as a rare manifestation of dermatomyositis: clinical lesson from a rare feature. J Clin Rheumatol. 2011; 17:135–7.14. Koler RA, Montemarano A. Dermatomyositis. Am Fam Physician. 2001; 64:1565–72.15. Castro C, Gourley M. Diagnosis and treatment of inflammatory myopathy: issues and management. Ther Adv Musculoskelet Dis. 2012; 4:111–20.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Overlap Syndrome with Rheumatoid Arthritis and Polymyositis
- Three Cases of Overlap Syndrome Consisting of Systemic Sclerosis and Rheumatoid Arthritis
- Systemic lupus erythematosus accompanied with idiopathic inflammatory myopathy: report of 2 cases
- A Case of Overlap Syndrome with Systemic Sclerosis and Rheumatoid Arthritis
- A Case of Diffuse Alveolar Hemorrhage Associated with Overlap syndrome
