Three Various Cases of Retinal Hemorrhages Caused by Plasmodium vivax Malaria
- Affiliations
-
- 1Department of Ophthalmology, Inha University Hospital, Inha University College of Medicine, Incheon, Korea. DrMYS@inha.ac.kr
- KMID: 2214713
- DOI: http://doi.org/10.3341/jkos.2011.52.7.863
Abstract
- PURPOSE
To report three various cases of retinal hemorrhages caused by Plasmodium vivax malaria.
CASE SUMMARY
Two 55-year-old male patients and a 52-year-old male patient with cyclic high fever were admitted to the department of internal medicine. Three of the patients were diagnosed with malaria caused by P. vivax based on a peripheral blood smear. The patients were treated with hydroxychloroquine and premaquine but complained of decreased visual acuity. The patients were examined with funduscopy, fluorescein angiography, and optical coherence tomography. The first case showed 2 areas of retinal hemorrhages on the macular in the right eye and 1 area of retinal hemorrhage in the left eye. The second case showed many cotton-wool spots along with a number of small retinal hemorrhages and tortuous blood vessels in both eyes. The third case showed 1 area of retinal hemorrhage in the right eye and many cotton-wool spots in both eyes.
CONCLUSIONS
P. vivax malaria rarely causes retinal hemorrhage. Manifestations of retinal hemorrhage and degree of visual acuity loss may vary among patients. P. vivax malaria should be considered when patients with unexplained high fever present with retinal hemorrhage, even without a history of overseas travel.
MeSH Terms
Figure
-
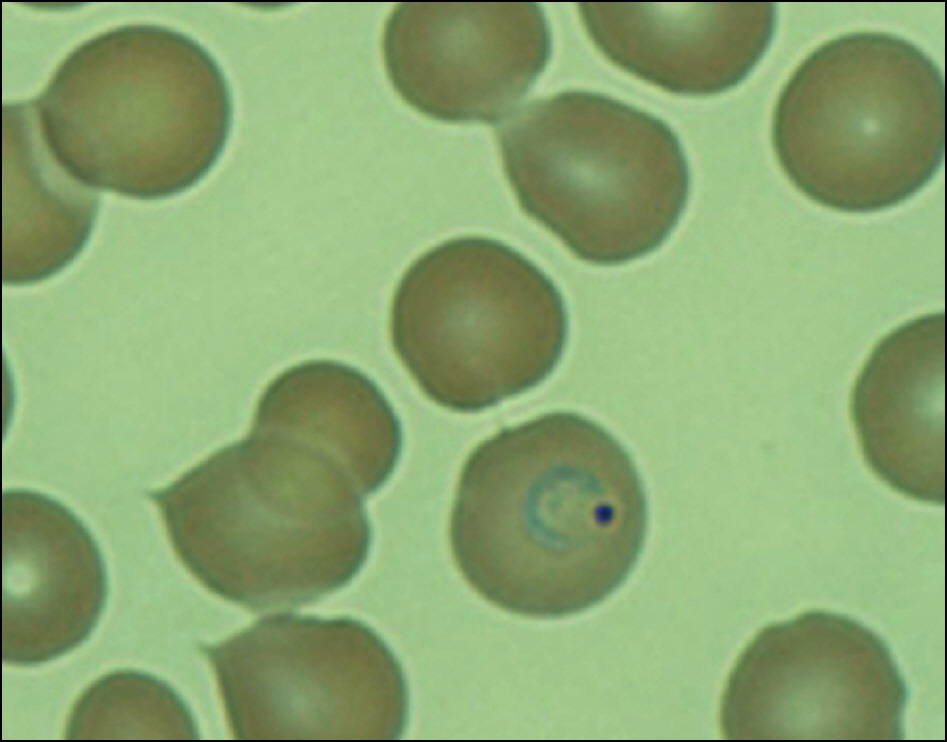
Figure 1. Case 1. Peripheral blood smears showing ring forms of trophozoite of Plasmodium vivax (Wright-Giemsa stain, ×1,000).
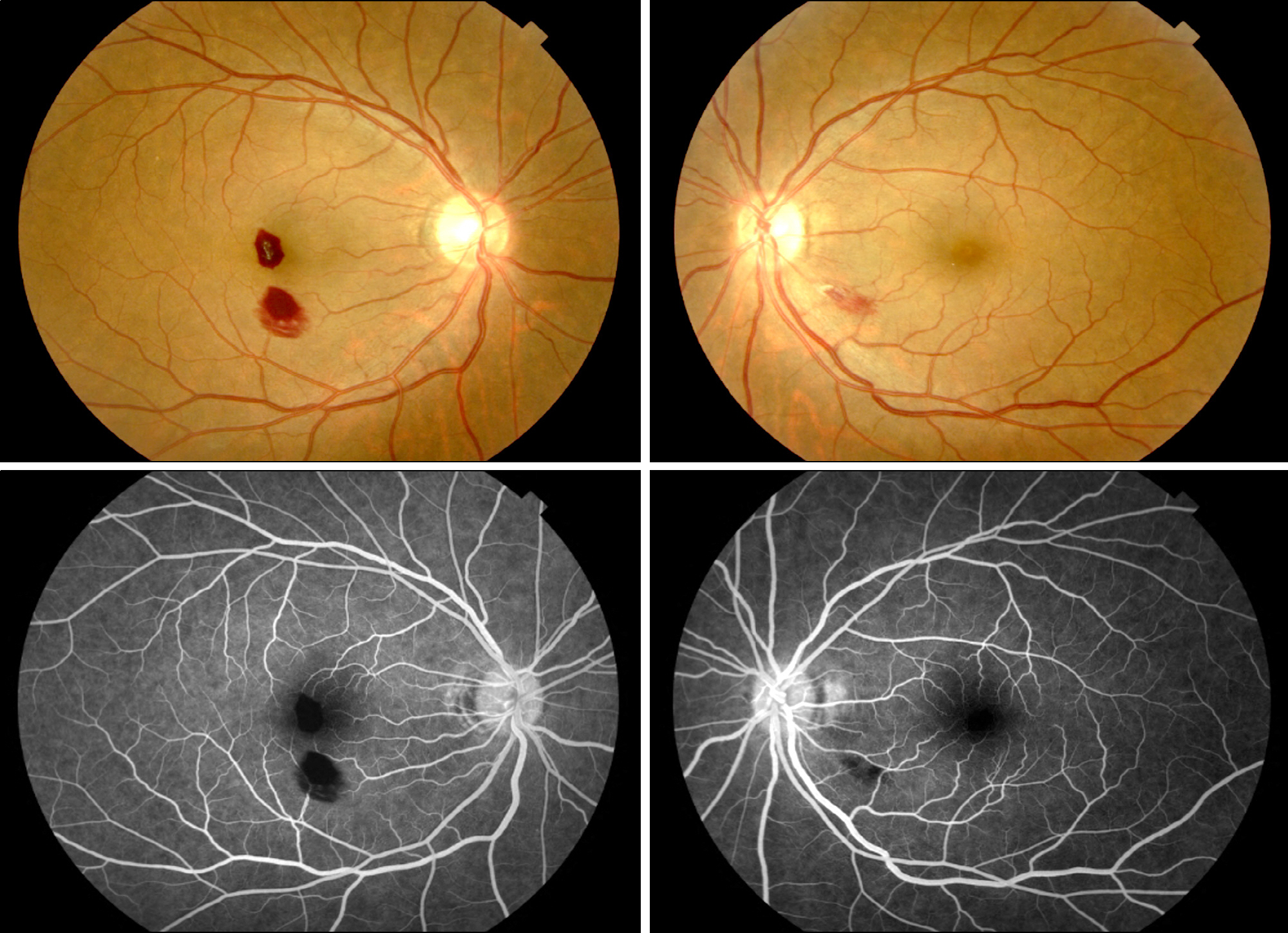
Figure 2. Case 1. Fundus photographs of a 52-years old male infected with Plasmodium vivax at presentation. Two retinal hemorrhages were found in the right eye, one of which was located at the macula and the other of which was inferior to the macula. In the left eye, one retinal hemorrhage with a cotton wool spot was found infernasal to the macula. Fluorescein angiography show blocked fluorescences in both eyes caused by retinal hemorrhages.
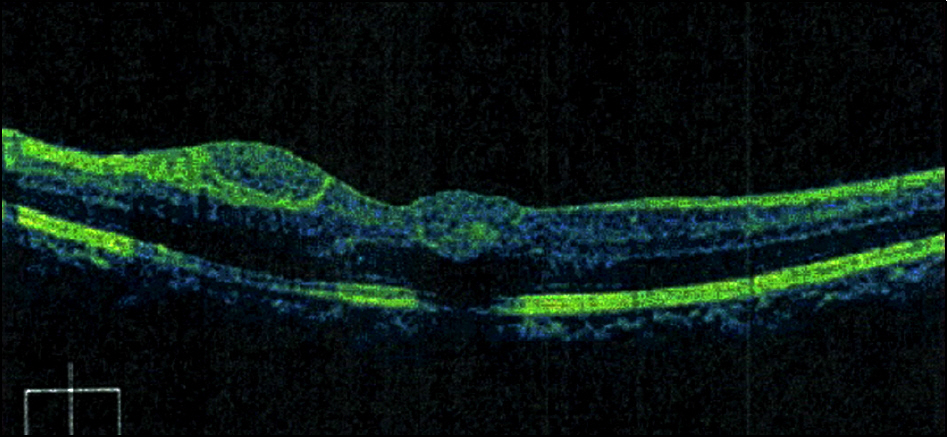
Figure 3. Case 1. Spectral domain optical coherence tomography. Central macular thickness was 328 μ m in the right eye. The locations of the hemorrhages were found to exist at the level of the intraretinal space.
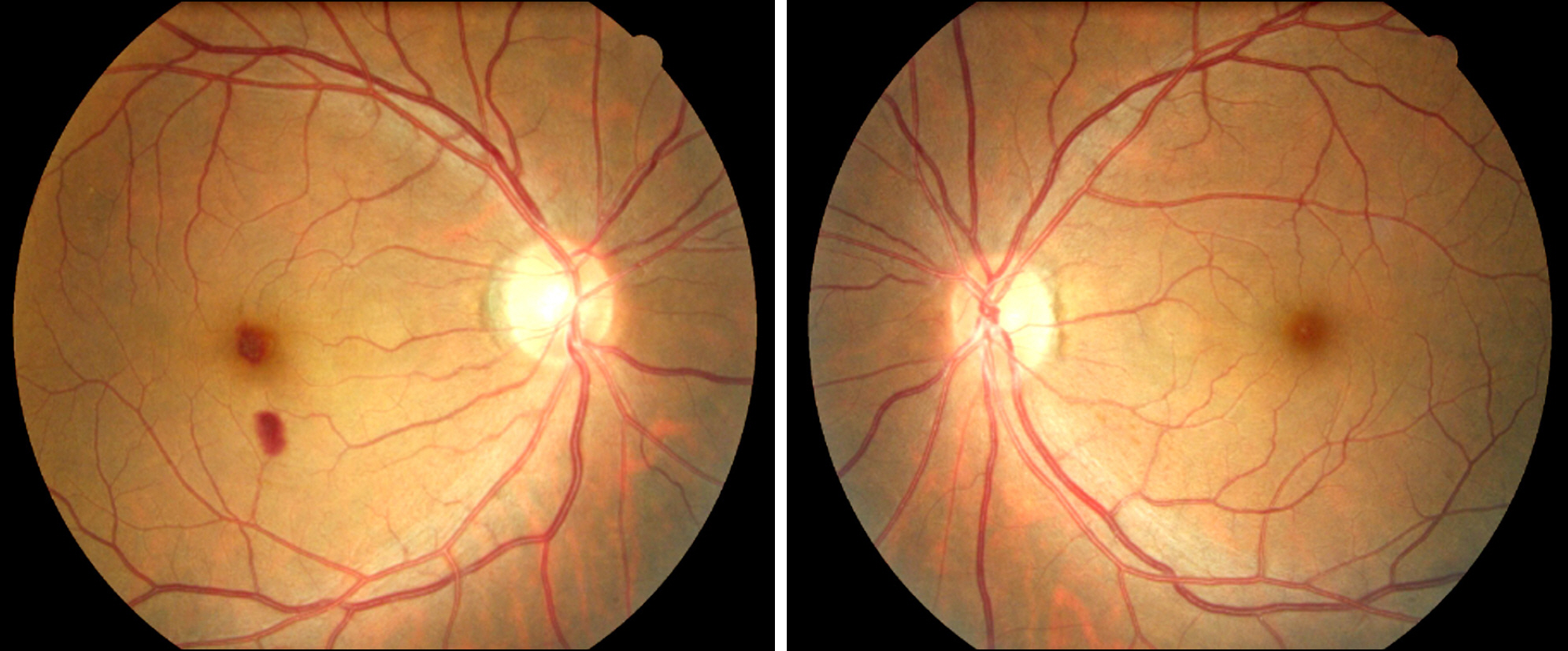
Figure 4. Case 1. Fundus photographs at 1 month after the onset of ocular symptoms. The initial retinal hemorrhage at the macula decreased in the right eye. The initial retinal hemorrhage was completely absorbed in the left eye.
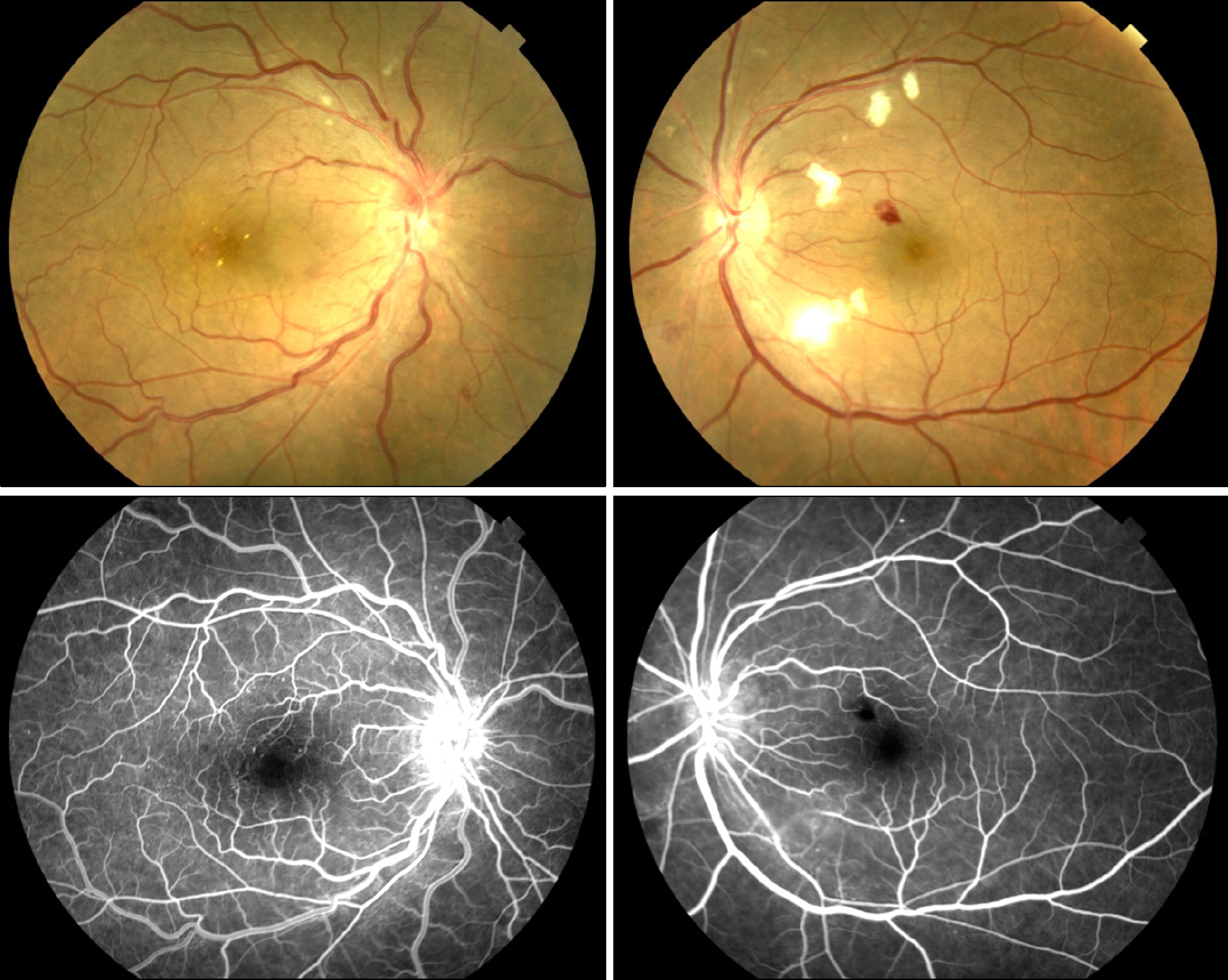
Figure 5. Case 2. The fundus photographs of a 55-years-old male infected with Plasmodium vivax at presentation. The fundus of the right eye shows tortous retinal vessels and multiple dot hemorrhages in the posterior pole. In the left eye, 1 area of retinal hemorrhage was found superonasal to the macula and multiple cotton wool spots were also found in the posterior pole. Fluorescein angiography shows tortous retinal vessels in the right eye. In the left eye, blocked fluorescence was caused by the retinal hemorrhages superonasal to the macula.
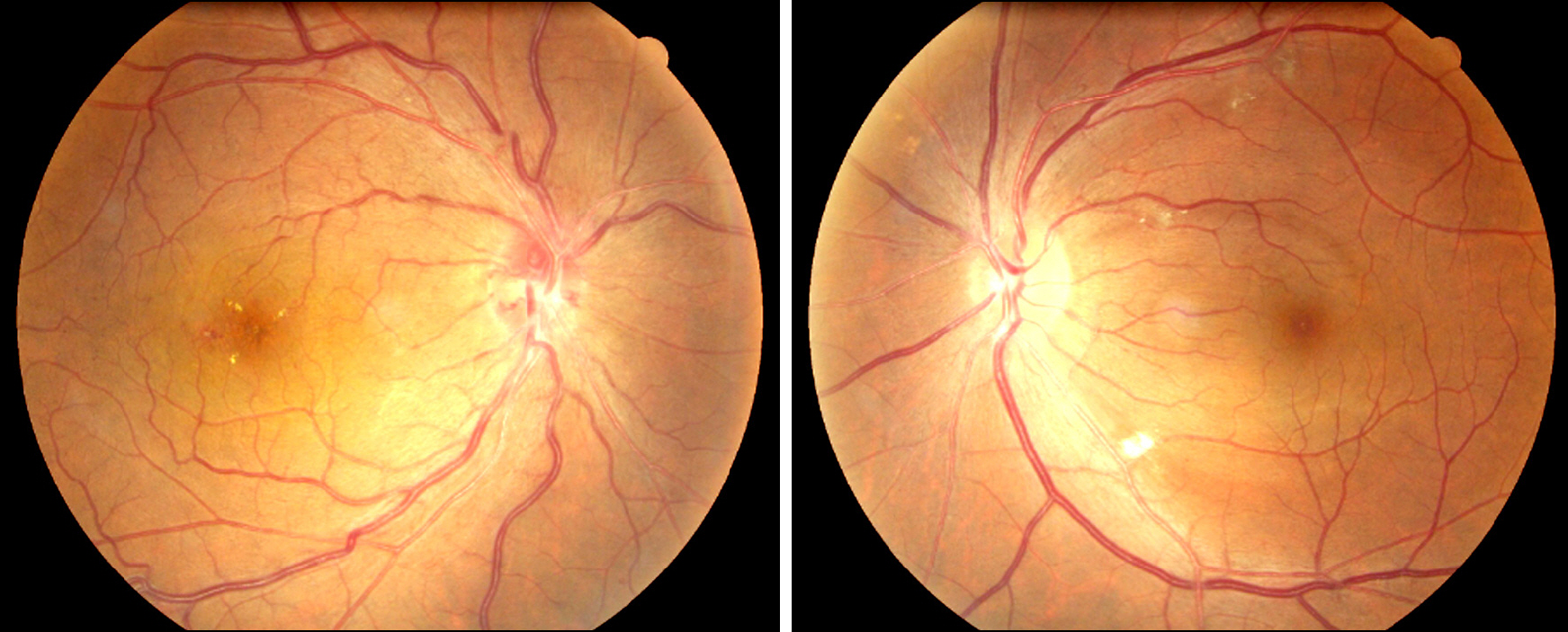
Figure 6. Case 2. Fundus photographs at 1 month after the onset of ocular symptoms. The initial retinal hemorrhage was completely absorbed in both eyes. The cotton wool spots were significantly decreased in both eyes.
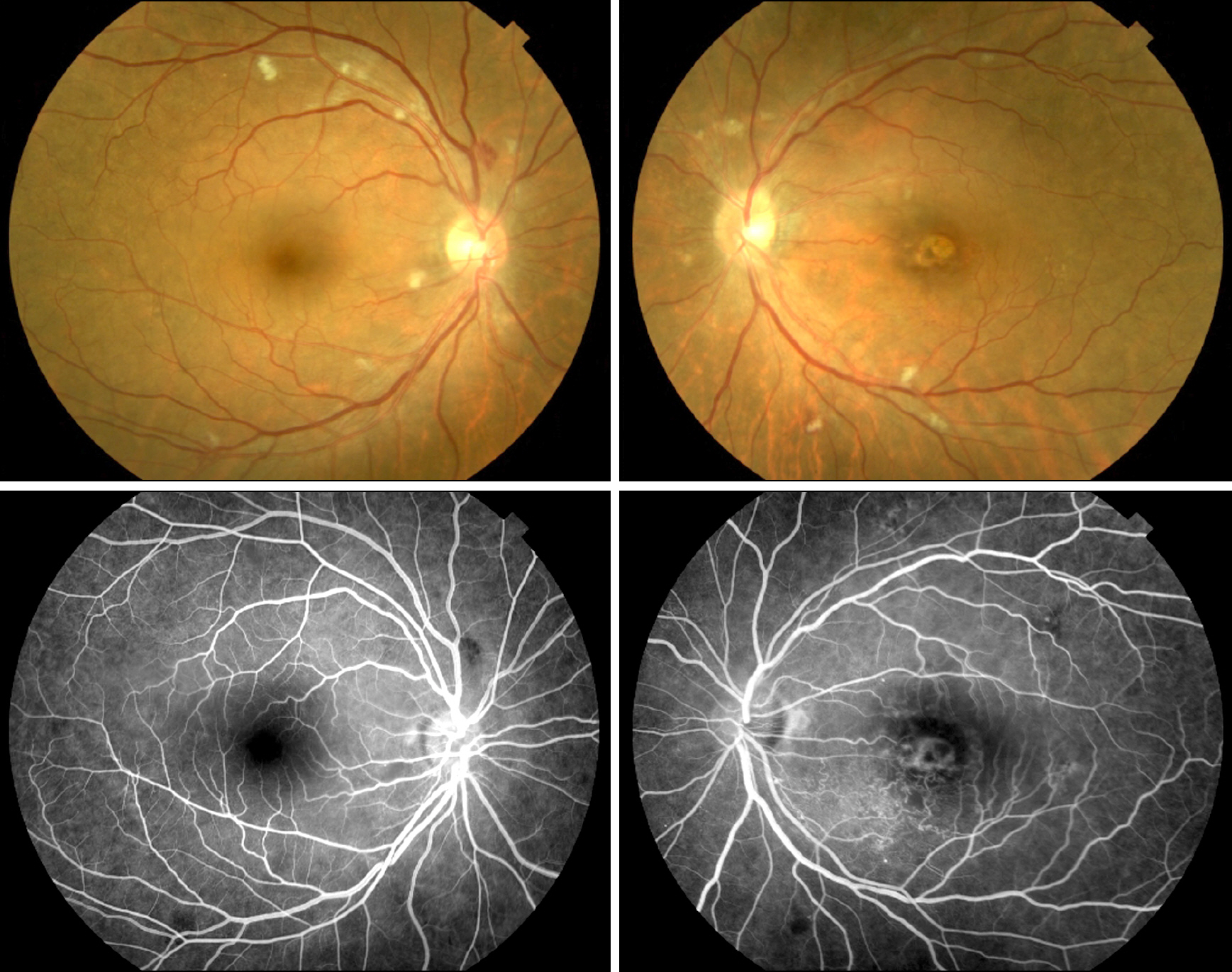
Figure 7. Case 3. Fundus photographs of a 55-years old male infected with Plasmodium vivax at presentation. The fundus of the right eye shows multiple cotton wool spots in the posterior pole and one area of retinal hemorrhage superior to the optic disc. In the left eye, multiple cotton wool spots were found in the posterior pole. Fluorescein angiography of the right eye shows blocked fluorescence caused by the retinal hemorrhage superior to the optic disc.
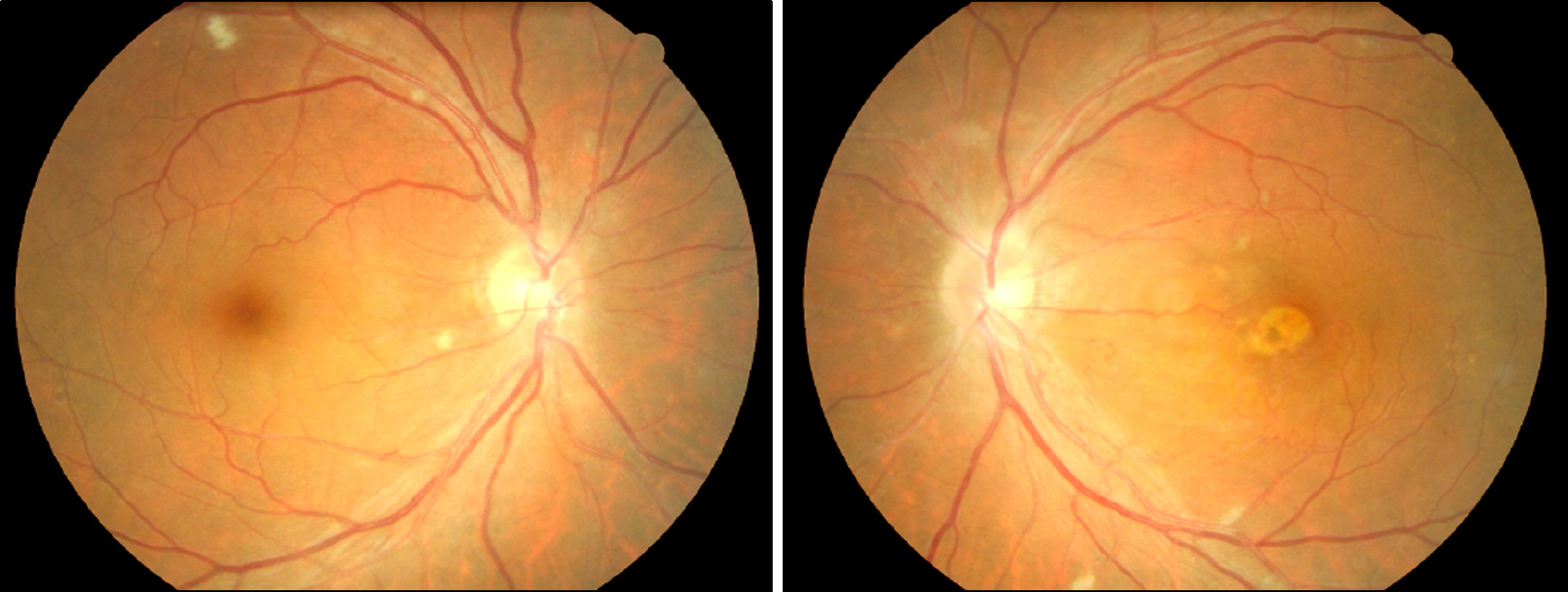
Figure 8. Case 3. Fundus photographs at 1 month after the onset of ocular symptoms. The initial retinal hemorrhage was completely absorbed in the right eye. The cotton wool spots significantly decreased in both eyes.
Reference
-
References
1. Kho WG. Reemergence of malaria in Korea. J Korean Med Assoc. 2007; 50:959–66.
Article2. Biswas J, Fogla R, Srinivasan P, et al. Ocular malaria. A clinical and histopathologic study. Ophthalmology. 1996; 103:1471–5.3. Beare NA, Taylor TE, Harding SP, et al. Malarial retinopathy: a newly established diagnostic sign in severe malaria. Am J Trop Med Hyg. 2006; 75:790–7.
Article4. Chai IH, Lim GI, Yoon SN, et al. Occurrence of tertian malaria in a male patient who has never been abroad. Korean J Parasitol. 1994; 32:195–200.
Article5. Cho SY, Kong Y, Park SM, et al. Two vivax malaria cases detected in Korea. Korean J Parasitol. 1994; 32:281–4.
Article6. Lee JS, Kho WG, Lee HW, et al. Current status of vivax malaria among civilians in Korea. Korean J Parasitol. 1998; 36:241–8.
Article7. Yi KJ, Chung MH, Kim HS, et al. A relapsed case of imported tertian malaria after a standard course of hydroxychloroquine and primaquine therapy. Korean J Parasitol. 1998; 36:143–6.
Article8. Mackintosh CL, Beeson JG, Marsh K. Clinical features and pathogenesis of severe malaria. Trends Parasitol. 2004; 20:597–603.
Article9. Looareesuwan S, Warrell DA, White NJ, et al. Retinal hemorrhage, a common sign of prognostic significance in cerebral malaria. Am J Trop Med Hyg. 1983; 32:911–5.10. Idro R, Jenkins NE, Newton CR. Pathogenesis, clinical features, and neurological outcome of cerebral malaria. Lancet Neurol. 2005; 4:827–40.
Article11. Maude RJ, Dondorp AM, Abu Sayeed A, et al. The eye in cerebral malaria: what can it teach us? Trans R Soc Trop Med Hyg. 2009; 103:661–4.
Article12. Hidayat AA, Nalbandian RM, Sammons DW, et al. The diagnostic histopathologic features of ocular malaria. Ophthalmology. 1993; 100:1183–6.
Article13. Choi HJ, Lee SY, Yang H, Bang JK. Retinal haemorrhage in vivax malaria. Trans R Soc Trop Med Hyg. 2004; 98:387–9.
Article14. Oh J, Kim HS, Huh K. Cerebral malaria associated with retinal hemorrhage on macular area. J Korean Ophthalmol Soc. 2003; 44:2699–704.15. Beare NA, Taylor TE, Harding SP, et al. Malarial retinopathy: a newly established diagnostic sign in severe malaria. Am J Trop Med Hyg. 2006; 75:790–7.
Article16. Beare NA, Southern C, Kayira K, et al. Visual outcomes in children in Malawi following retinopathy of severe malaria. Br J Ophthalmol. 2004; 88:321–4.
Article17. Nagpal KC, Goldberg MF, Rabb MF. Ocular manifestations of sickle hemoglobinopathies. Surv Ophthalmol. 1977; 21:391–411.
Article18. Choy YJ, Park JS. A Case of bilateral retinal hemorrhages caused by plasmodium vivax malaria. J Korean Ophthalmol Soc. 2010; 51:626–30.
Article19. Beare NA, Southern C, Chalira C, et al. Prognostic significance and course of retinopathy in children with severe malaria. Arch Ophthalmol. 2004; 122:1141–7.20. Hidayat AA, Nalbandian RM, Sammons DW, et al. The diagnostic histopathologic features of ocular malaria. Ophthalmology. 1993; 100:1183–6.
Article21. Lou J, Lucas R, Grau GE. Pathogenesis of cerebral malaria: recent experimental data and possible applications for humans. Clin Microbiol Rev. 2001; 14:810–20.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Bilateral Retinal Hemorrhages Caused by Plasmodium Vivax Malaria
- Retinal Hemorrhage in an Adult with P. vivax Malaria
- A Case of Plasmodium Vivax Malaria with Cerebral Complications
- A case of Plasmodium vivax malaria occurring during a school excursion to Pocheon-gun
- Multiple Cerebral Infarcts Following Acute Plasmodium vivax Infection
