A Case of Fusarium Deep Keratitis Following Scleral Graft
- Affiliations
-
- 1Department of Ophthalmology, Chung-Ang University College of Medicine, Seoul, Korea. yschun100@hanmail.net
- KMID: 2213406
- DOI: http://doi.org/10.3341/jkos.2010.51.4.606
Abstract
- PURPOSE
To report a case of drug-resistant Fusarium deep keratitis following sclera graft.
CASE SUMMARY
A 48-year-old woman, who underwent excision of the pterygium nine years previous, received a scleral graft for scleromalacia and ocular pain. After surgery, due to melting of the scleral graft and the presence of Fusarium deep keratitis, she received surgical and intensive medical treatment including three intracameral injections of antifungal agent, administration of topical voriconazole 1%, scleral re-graft, autologous conjunctival graft, and amniotic membrane transplantation. Nevertheless, the patient's ocular condition deteriorated with increased hypopyon, corneal opacity, and perforation. Enucleation was ultimately performed.
Keyword
MeSH Terms
Figure
-
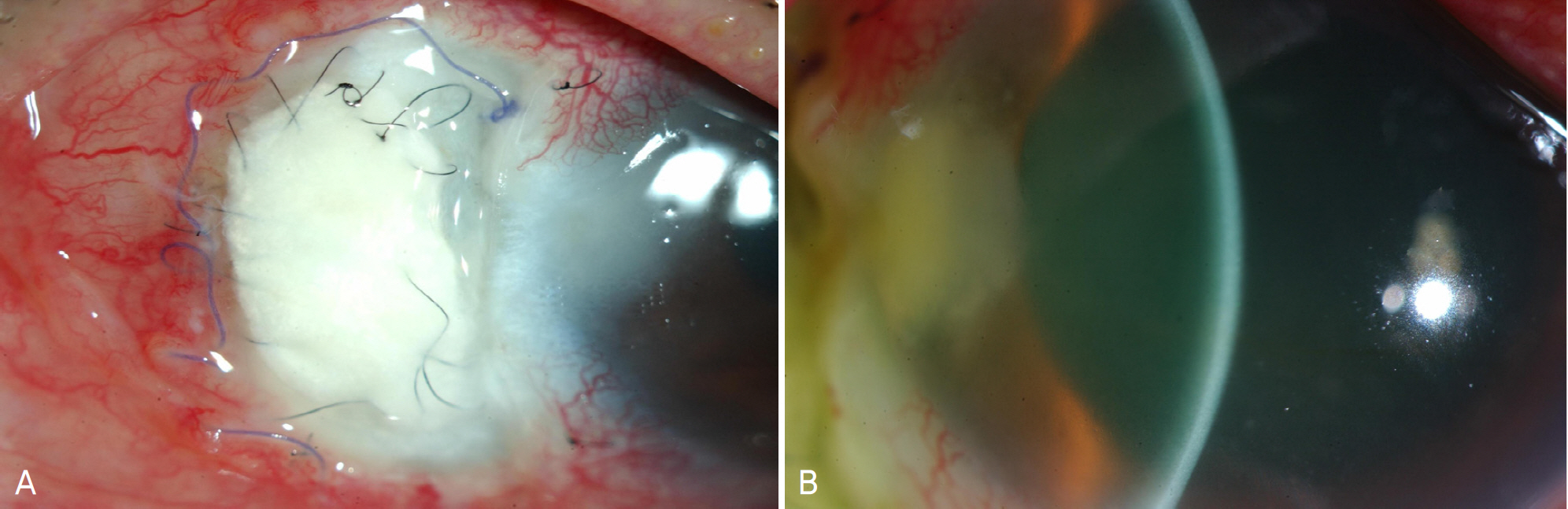
Figure 1. (A) At the diagnosis, there was severe melting of scleral graft and its surrounding tissue with severe conjuncitval injection. Corneal ulcer spread out from the necrotic sclera. (B) 1×2 mm round soft whitish mass was observed behind the stromal infiltration.
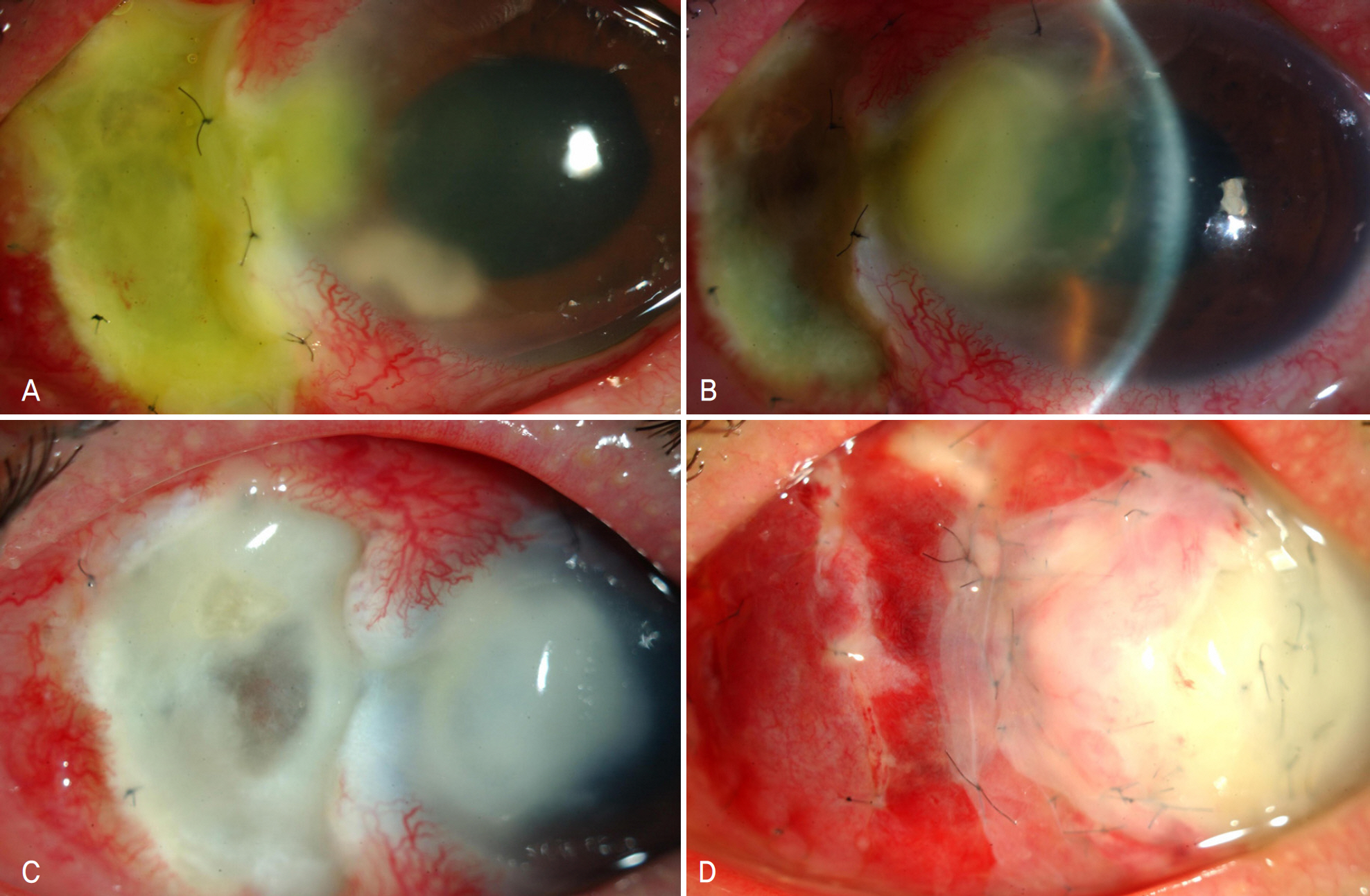
Figure 2. Color photographs of progression. (A) At 3 days after treatment, corneal infiltration was stationary but 2×2mm whitish mass developed again. (B) At 7 days after treatment, increased corneal ulcer with immune ring and aggravated sclera melting were found. (C) At 13 days after treatment, dense corneal infilration with enlarged scleral melting (5×4 mm) was observed. (D) At 17 days after treatment, although scleral graft, autologous conjunctival graft, and amniotic membrane transplantation were performed but yellow necrotized corneal ulcer developed at total cornea.

Figure 3. At 10 days after culture of aqueous humor and sclera, Fusarium solani was cultured. (A) Orange colored colony with lighter periphery on Sabouraud's agar plate. (B) There are two types of sporulation; large, sickle shaped, multiseptated macroconidia and small, oval shaped, microconidia in clusters.
Cited by 4 articles
-
A Case of Endophthalmitis Treated with Surgical Removal of the Inflammatory Plaque on Corneal Endothelium
Nam Kyun Koo, Kwang Soo Kim, Yu Cheol Kim
J Korean Ophthalmol Soc. 2011;52(8):990-993. doi: 10.3341/jkos.2011.52.8.990.Clinical Effects of Intracameral Voriconazole Injection in Patients with Fungal Keratitis Refractory to Conventional Treatment
Se Hyeong Jeong, Hyo Seok Lee, Jae Kap Cho, Kyung Chul Yoon
J Korean Ophthalmol Soc. 2013;54(5):696-703. doi: 10.3341/jkos.2013.54.5.696.A Case of Fungal Keratitis Caused by Paecilomyces lilacinus after Penetrating Keratoplasty
Jae Yon Won, Ji Young Shin, Je Hyung Hwang, Choun-Ki Joo
J Korean Ophthalmol Soc. 2014;55(9):1384-1387. doi: 10.3341/jkos.2014.55.9.1384.Treatment of Scleromalacia with Scleral Autograft
Young Jin Song, Seung Il Jung, Ji Won Kwon
J Korean Ophthalmol Soc. 2014;55(11):1706-1709. doi: 10.3341/jkos.2014.55.11.1706.
Reference
-
References
1. Sharma S, Srinivasan M, Upadhyay MP. Corneal blindness: a global perspective. Bull World Health Organ. 2001; 79:214–21.2. Thomas PA. Mycotic keratitis – an underestimated mycosis. J Med Vet Mycol. 1994; 32:235–56.
Article3. Jay HK, Mark JM, Edward JH. Cornea and external disease: Clinical diagnosis and management. 2. St. Louis: CV Mosby;1997. p. 1253–65.4. Verma S, Tuft SJ. Fusarium solani keratitis following LASIK for myopia. Br J Ophthalmol. 2002; 86:1190–1.
Article5. Abad JC, Foster CS. Fungal keratitis. Int Ophthalmol Clin. 1996; 36:1–15.
Article6. Kim YS, Song YS, Kim JC. Fungal Keratitis Caused by Chromomycetes. J Korean Ophthalmol Soc. 2003; 44:755–9.7. Frota AC, Lima Filho AA, Dias AB, et al. Freeze-drying as an abdominal method of human sclera preservation. Arq Bras Oftalmol. 2008; 71:137–41.8. Lusky M, Weinreb RN. Preservation of Scleral Graft to avoid HIV infection. J Glaucoma. 1992; 1:221.9. O'Day DM, Ray WA, Robinson RD, Head WS. Efficacy of abdominal agents in the cornea, Ⅱ: influence of corticosteroids. Invest Ophthalmol Vis Sci. 1984; 25:331–5.10. O'Day DM, Ray WA, Head WS. Influence of corticosteroid on experimentally induced keratomycosis. Arch Ophthalmol. 1991; 109:1601–4.11. Kaushik S, Ram J, Brar GS, et al. Intracameral amphotericin B abdominal experience in severe keratomycosis. Cornea. 2001; 20:715–9.12. Kuriakose T, Kothari M, Paul P, et al. Intracameral amphotericin B injection in the management of deep keratomycosis. Cornea. 2002; 21:653–6.
Article13. Reis A, Sundmacher R, Tintelnot K, et al. Successful treatment if ocular invasive mould infection (fusariosis) with the new abdominal agent voriconazole. Br J Ophthalmol. 2000; 84:932–3.14. Yoon JU, Kim SW, Ha BJ, et al. A case of fungal keratitis treated with voriconazole. J Korean Ophthalmol Soc. 2008; 49:1680–4.
Article15. Banitt M, Berenbom A, Shah M, et al. A case of polymicrobial abdominal violating an intact lens capsule. Cornea. 2008; 27:1057–61.16. Tu EY, McCartney DL, Beatty RF, et al. Successful treatment of resistant ocular fusariosis with posaconazole. Am J Ophthalmol. 2007; 143:222–7.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Fusarium solani Keratitis mixed by Acremonium falciforme
- Clinical Aspect and Prognosis of Staphylococcus Epidermidis Keratitis
- A Case of Fusarium Keratitis Treated with Moxifloxacin 0.5% Ophthalmic Solution
- Three Cases of Secondary Fungal Infection in Herpes Simplex Keratitis
- A Case Report of Intracameral Amphotericin B Injection in the Management of Deep Keratomycosis
