J Korean Ophthalmol Soc.
2012 Feb;53(2):338-341.
A Case of Fusarium Keratitis Treated with Moxifloxacin 0.5% Ophthalmic Solution
- Affiliations
-
- 1Department of Ophthalmology, Keimyung University School of Medicine, Daegu, Korea. sdchang@dsmc.or.kr
- 2Eye Clinic of Jukjeon, Daegu, Korea.
Abstract
- PURPOSE
To report a case of fusarium keratitis treated with only moxifloxacin 0.5% ophthalmic solution (Vigamox(R), Alcon Laboratories, Inc., Ft Worth, TX, USA).
CASE SUMMARY
A 37-year-old healthy male patient experienced a right eye injury due to grain 7 days prior to presentation at our hospital with visual disturbance and ocular pain. A 2.7 x 4.3 mm sized corneal epithelial defect with irregular featherlike midstromal infiltration was observed, and slit lamp examination revealed a dry, rough texture. Thus a smear and culture were performed. Moxifloxacin 0.5% ophthalmic solution (Vigamox(R)) and lubricant were applied for treatment. Three days after using the eye solution, all clinical features improved. Seven days later, Fusarium species was identified in culture.
CONCLUSIONS
As standard treatment for Fusarium, the authors of the present study used an antifungal agent. Although hyphae were detected in culture, the use of only moxifloxacin 0.5% ophthalmic solution (Vigamox(R)) result in a satisfactory result and improvement in clinical features.
Keyword
MeSH Terms
Figure
-
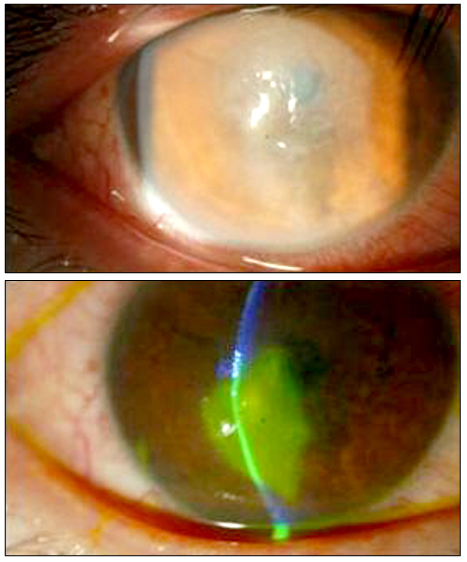
Figure 1 Pretherapeutic photographs.
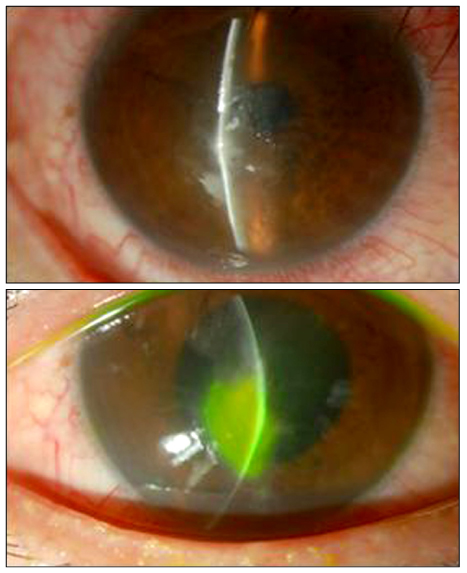
Figure 2 Post-theraupetic photographs (3 days).
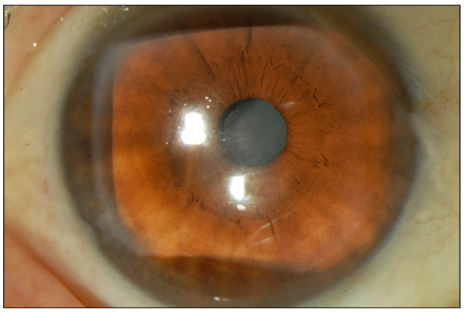
Figure 3 Post-theraupetic photographs (1 month).
Reference
-
1. Srinivasan M. Fungal keratitis. Curr Opin Ophthalmol. 2004. 15:321–327.2. O'Day DM. Selection of appropriate antifungal therapy. Cornea. 1987. 6:238–245.3. Kim YS, Song YS, Kim JC. Fungal keratitis caused by chromomycetes. J Korean Ophthalmol Soc. 2003. 44:755–759.4. O'Day DM, Ray WA, Robinson RD, Head WS. Efficacy of antifungal agents in the cornea. II. Influence of corticosteroids. Invest Ophthalmol Vis Sci. 1984. 25:331–335.5. O'Day DM, Ray WA, Head WS, et al. Influence of corticosteroid on experimentally induced keratomycosis. Arch Ophthalmol. 1991. 109:1601–1604.6. Whitcher JP, Srinivasan M, Upadhyay MP. Coneal blindness: a global perspective. Bull World Health Organ. 2001. 79:214–221.7. Thomas PA. Mycotic keratitis--an underestimated mycosis. J Med Vet Mycol. 1994. 32:235–256.8. Wong TY, Ng TP, Fong KS, Tan DT. Risk factors and clinical outcomes between fungal and bacterial keratitis: a comparative study. CLAO J. 1997. 23:275–281.9. Lee KH, Chae HJ, Yoon KC. Analysis of risk factors for treatment failure in fungal keratitis. J Korean Ophthalmol Soc. 2008. 49:737–742.10. Day S, Lalitha P, Haug S, et al. Activity of antibiotics against Fusarium and Aspergillus. Br J Ophthalmol. 2009. 93:116–119.11. Dalhoff A, Shalit I. Immunomodulatory effects of quinolones. Lancet Infect Dis. 2003. 3:359–371.12. Nitiss JL. Investigating the biological functions of DNA topoisomerases in eukaryotic cells. Biochim Biophys Acta. 1998. 1400:63–81.13. Munir WM, Rosenfeld SI, Udell I, et al. Clinical response of contact lens-associated fungal keratitis to topical fluoroquinolone theraphy. Cornea. 2007. 26:621–624.14. Jay HK, Mark JM, Edward JH. Cornea and External Disease: Clinical Diagnosis and Management. 1997. St. Louis: CV Mosby;1253–1265.15. Verma S, Tuft SJ. Fusarium solani keratitis following LASIK for myopia. Br J Ophthalmol. 2002. 86:1190–1191.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Fusarium solani Keratitis mixed by Acremonium falciforme
- A Case of Allergic Reaction to 0.5% Moxifloxacin Eye Drops
- Moxifloxacin Mixed Augmented Amniotic Membrane Transplantation for Perforating Infectious Keratitis
- A Case of Fusarium Deep Keratitis Following Scleral Graft
- A Case of Acinetobacter Baumannii Keratitis After Contact Lens Wearing
