Renal and abdominal visceral complications after open aortic surgery requiring supra-renal aortic cross clamping
- Affiliations
-
- 1Division of Vascular Surgery, Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. ywkim@skku.edu
- KMID: 2212289
- DOI: http://doi.org/10.4174/jkss.2012.83.3.162
Abstract
- PURPOSE
The aim of this study was to assess renal or abdominal visceral complications after open aortic surgery (OAS) requiring supra-renal aortic cross clamping (SRACC).
METHODS
We retrospectively reviewed the medical records of 66 patients who underwent SRACC. Among them, 17 followed supra-celiac aortic cross clamping (SCACC) procedure, 42 supra-renal, and 7 inter-renal aorta. Postoperative renal, hepatic or pancreatic complications were investigated by reviewing levels of serum creatinine and hepatic and pancreatic enzymes. Preoperative clinical and operative variables were analyzed to determine risk factors for postoperative renal insufficiency (PORI).
RESULTS
Indications for SRACC were 25 juxta-renal aortic occlusion and 41 aortic aneurysms (24 juxta-renal, 12 supra-renal and 5 type IV thoraco-abdominal). The mean duration of renal ischemic time (RIT) was 30.1 +/- 22.2 minutes (range, 3 to 120 minutes). PORI developed in 21% of patients, including four patients requiring hemodialysis (HD). However, chronic HD was required for only one patient (1.5%) who had preoperative renal insufficiency. RIT > or = 25 minutes and SCACC were significant risk factors for PORI development by univariate analysis, but not by multivariate analysis. Serum pancreatic and hepatic enzyme was elevated in 41% and 53% of the 17 patients who underwent SCACC, respectively.
CONCLUSION
Though postoperative renal or abdominal visceral complications developed often after SRACC, we found that most of those complications resolved spontaneously unless there was preexisting renal disease or the aortic clamping time was exceptionally long.
Keyword
MeSH Terms
Figure
-
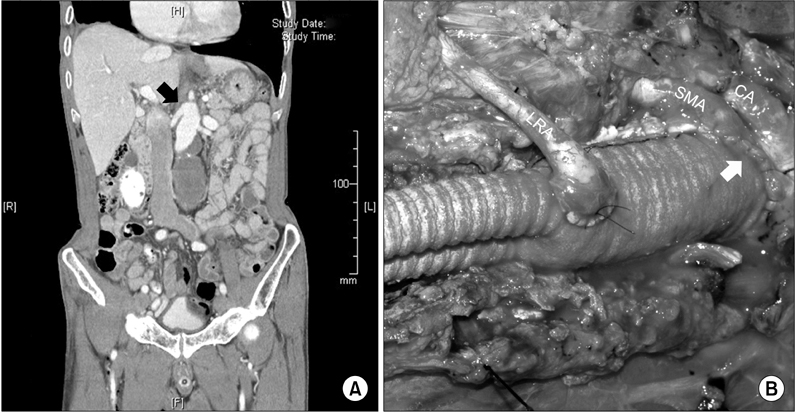
Fig. 1 (A) Computed tomography angiogram of supra-renal abdominal aortic aneurysm (AAA) (black arrow), which involves the origin of both renal arteries. (B) Surgical photograph showing suprarenal AAA repair, which includes the proximal aortic anastomosis performed via the inclusion technique (white arrow) and concomitant left renal artery reimplantation to the aortic prosthetic graft. CA, celiac artery; SMA, superior mesenteric artery; LRA, left renal artery.
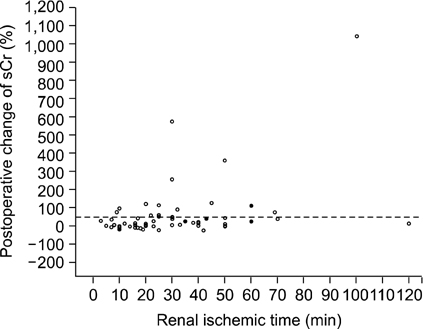
Fig. 2 A scatter plots showing postoperative change of the serum creatinine level according to the renal ischemic time. Empty circles (○) denote patients who did not undergo renal hypothermia; solid circles (•) denote patients who underwent renal hypothermia during the suprarenal aortic cross clamping. sCr, serum creatinine.
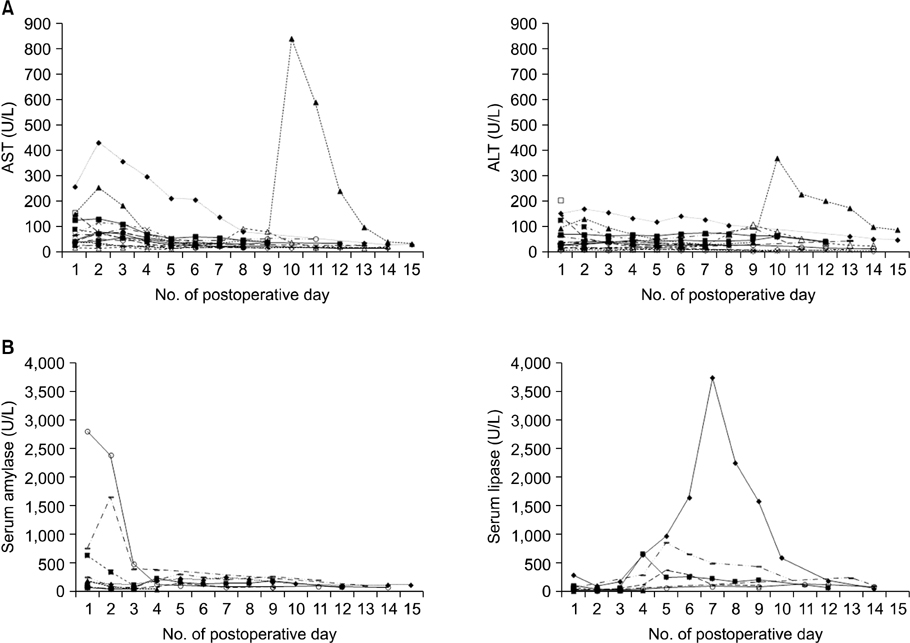
Fig. 3 Postoperative serum hepatic (A) and pancreatic enzyme (B) levels in patients who underwent aortic surgery requiring supra-celiac aortic cross clamping (n = 17). AST, aspartate aminotransferase; ALT, alanine aminotransferase.
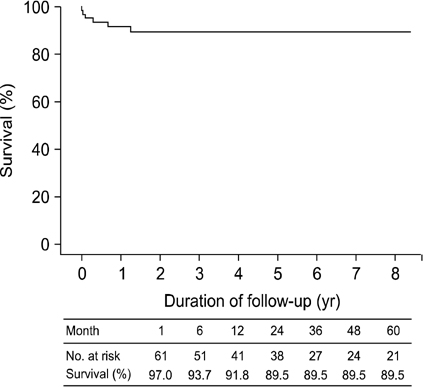
Fig. 4 Postoperative survival of 66 patients who underwent supra-renal aortic cross clamping (Kaplan-Meier curve).
Reference
-
1. Costin JA, Watson DR, Duff SB, Edmonson-Holt A, Shaffer L, Blossom GB. Evaluation of the complexity of open abdominal aneurysm repair in the era of endovascular stent grafting. J Vasc Surg. 2006. 43:915–920.2. Park YJ, Kim N, Kim YW. Investigation of current trend of AAA treatment in Korea. J Korean Surg Soc. 2011. 80:125–130.3. Kim TH, Ko YG, Kim U, Kim JS, Choi D, Hong MK, et al. Outcomes of endovascular treatment of chronic total occlusion of the infrarenal aorta. J Vasc Surg. 2011. 53:1542–1549.4. Sharp WJ, Bashir M, Word R, Nicholson R, Bunch C, Corson J, et al. Suprarenal clamping is a safe method of aortic control when infrarenal clamping is not desirable. Ann Vasc Surg. 2008. 22:534–540.5. Giulini SM, Bonardelli S, Portolani N, Giovanetti M, Galvani G, Maffeis R, et al. Suprarenal aortic cross clamping in elective abdominal aortic aneurysm surgery. Eur J Vasc Endovasc Surg. 2000. 20:286–289.6. Marrocco-Trischitta MM, Melissano G, Kahlberg A, Vezzoli G, Calori G, Chiesa R. The impact of aortic clamping site on glomerular filtration rate after juxtarenal aneurysm repair. Ann Vasc Surg. 2009. 23:770–777.7. Chong T, Nguyen L, Owens CD, Conte MS, Belkin M. Suprarenal aortic cross-clamp position: a reappraisal of its effects on outcomes for open abdominal aortic aneurysm repair. J Vasc Surg. 2009. 49:873–880.8. Kirby LB, Rosenthal D, Atkins CP, Brown GA, Matsuura JH, Clark MD, et al. Comparison between the transabdominal and retroperitoneal approaches for aortic reconstruction in patients at high risk. J Vasc Surg. 1999. 30:400–405.9. Martin GH, O'Hara PJ, Hertzer NR, Mascha EJ, Krajewski LP, Beven EG, et al. Surgical repair of aneurysms involving the suprarenal, visceral, and lower thoracic aortic segments: early results and late outcome. J Vasc Surg. 2000. 31:851–862.10. Michalopoulos A, Alivizatos P, Geroulanos S. Hepatic dysfunction following cardiac surgery: determinants and consequences. Hepatogastroenterology. 1997. 44:779–783.11. Hashimoto L, Walsh RM. Acute pancreatitis after aortic surgery. Am Surg. 1999. 65:423–426.12. Greenberg R, Eagleton M, Mastracci T. Branched endografts for thoracoabdominal aneurysms. J Thorac Cardiovasc Surg. 2010. 140:6 Suppl. S171–S178.13. Bruen KJ, Feezor RJ, Daniels MJ, Beck AW, Lee WA. Endovascular chimney technique versus open repair of juxtarenal and suprarenal aneurysms. J Vasc Surg. 2011. 53:895–904.14. Barshes NR, McPhee J, Ozaki CK, Nguyen LL, Menard MT, Gravereaux E, et al. Increasing complexity in the open surgical repair of abdominal aortic aneurysms. Ann Vasc Surg. 2012. 26:10–17.15. Wahlgren CM, Piano G, Desai T, Shaalan W, Bassiouny H. Transperitoneal versus retroperitoneal suprarenal cross-clamping for repair of abdominal aortic aneurysm with a hostile infrarenal aortic neck. Ann Vasc Surg. 2007. 21:687–694.16. Sasaki T, Ohsawa S, Ogawa M, Mukaida M, Nakajima T, Komoda K, et al. Postoperative renal function after an abdominal aortic aneurysm repair requiring a suprarenal aortic cross-clamp. Surg Today. 2000. 30:33–36.17. Shortell CK, Johansson M, Green RM, Illig KA. Optimal operative strategies in repair of juxtarenal abdominal aortic aneurysms. Ann Vasc Surg. 2003. 17:60–65.18. Wahlberg E, Dimuzio PJ, Stoney RJ. Aortic clamping during elective operations for infrarenal disease: the influence of clamping time on renal function. J Vasc Surg. 2002. 36:13–18.19. Knott AW, Kalra M, Duncan AA, Reed NR, Bower TC, Hoskin TL, et al. Open repair of juxtarenal aortic aneurysms (JAA) remains a safe option in the era of fenestrated endografts. J Vasc Surg. 2008. 47:695–701.20. West CA, Noel AA, Bower TC, Cherry KJ Jr, Gloviczki P, Sullivan TM, et al. Factors affecting outcomes of open surgical repair of pararenal aortic aneurysms: a 10-year experience. J Vasc Surg. 2006. 43:921–927.21. Green RM, Ricotta JJ, Ouriel K, DeWeese JA. Results of supraceliac aortic clamping in the difficult elective resection of infrarenal abdominal aortic aneurysm. J Vasc Surg. 1989. 9:124–134.22. Sarac TP, Clair DG, Hertzer NR, Greenberg RK, Krajewski LP, O'Hara PJ, et al. Contemporary results of juxtarenal aneurysm repair. J Vasc Surg. 2002. 36:1104–1111.23. Regner KR, Roman RJ. Role of medullary blood flow in the pathogenesis of renal ischemia-reperfusion injury. Curr Opin Nephrol Hypertens. 2012. 21:33–38.24. Zacharias M, Conlon NP, Herbison GP, Sivalingam P, Walker RJ, Hovhannisyan K. Interventions for protecting renal function in the perioperative period. Cochrane Database Syst Rev. 2008. (4):CD003590.25. Folkow B, Neil E. Circulation. 1971. New York: Oxford University Press.26. Anagnostopoulos PV, Shepard AD, Pipinos II, Raman SB, Chaudhry PA, Mishima T, et al. Hemostatic alterations associated with supraceliac aortic cross clamping. J Vasc Surg. 2002. 35:100–108.27. Nypaver TJ, Shepard AD, Reddy DJ, Elliott JP Jr, Ernst CB. Supraceliac aortic cross clamping: determinants of outcome in elective abdominal aortic reconstruction. J Vasc Surg. 1993. 17:868–875.28. Burkey SH, Valentine RJ, Jackson MR, Modrall JG, Clagett GP. Acute pancreatitis after abdominal vascular surgery. J Am Coll Surg. 2000. 191:373–380.29. Achouh PE, Madsen K, Miller CC 3rd, Estrera AL, Azizzadeh A, Dhareshwar J, et al. Gastrointestinal complications after descending thoracic and thoracoabdominal aortic repairs: a 14-year experience. J Vasc Surg. 2006. 44:442–446.30. Gullo L, Cavicchi L, Tomassetti P, Spagnolo C, Freyrie A, D'Addato M. Effects of ischemia on the human pancreas. Gastroenterology. 1996. 111:1033–1038.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Merits of and Technical Tips for Supra-Mesenteric Aortic Cross Clamping
- Hybrid Surgery for Supra-renal Abdominal Aortic Aneurysm: A case report
- Renal autotransplantation in open surgical repair of suprarenal abdominal aortic aneurysm
- Cardiac Arrest after Aortic Cross Clamping during Surgery for an Abdominal Aortic Aneurysm in a Patient with Coronary Artery Disease and Aortic Regurgitation: A Case Report
- Middle Aortic Syndrome with Superior Mesenteric and Bilateral Renal Artery Involvement: Unusual Type of Aortic Coarctation
