Upper Cervical Spine Injury
- Affiliations
-
- 1Department of Orthopaedic Surgery, Yonsei University, Wonju College of Medicine, Wonju, Korea. par73@yonsei.ac.kr
- KMID: 2209635
- DOI: http://doi.org/10.4184/jkss.2008.15.4.290
Abstract
- Upper cervical spine injuries, including atlantooccipital articulation, are being recognized more commonly and there is an increasing number of reports of patients surviving with injuries previously thought to be fatal. The bony elements of the upper cervical spine consist of the occiput, atlas and axis. The nature of their articulations provides no inherent stability, but rather relies on ligaments to maintain the structural integrity. Some upper cervical injuries, occipitocervical injuries, and isolated midsubstance transverse ligament ruptures, are usually unstable and frequently result in neurological injury or death. Therefore, these injuries warrant early instrumented posterior arthrodesis. Most upper cervical spine injuries can be treated non-surgically and heal readily. Implementation of a diagnostic algorithm consisting of screening parameters gathered from the plain radiographs as well as routine CT and MRI scans in high risk patients should reduce the occurrence of missed injuries.
Keyword
MeSH Terms
Figure
-
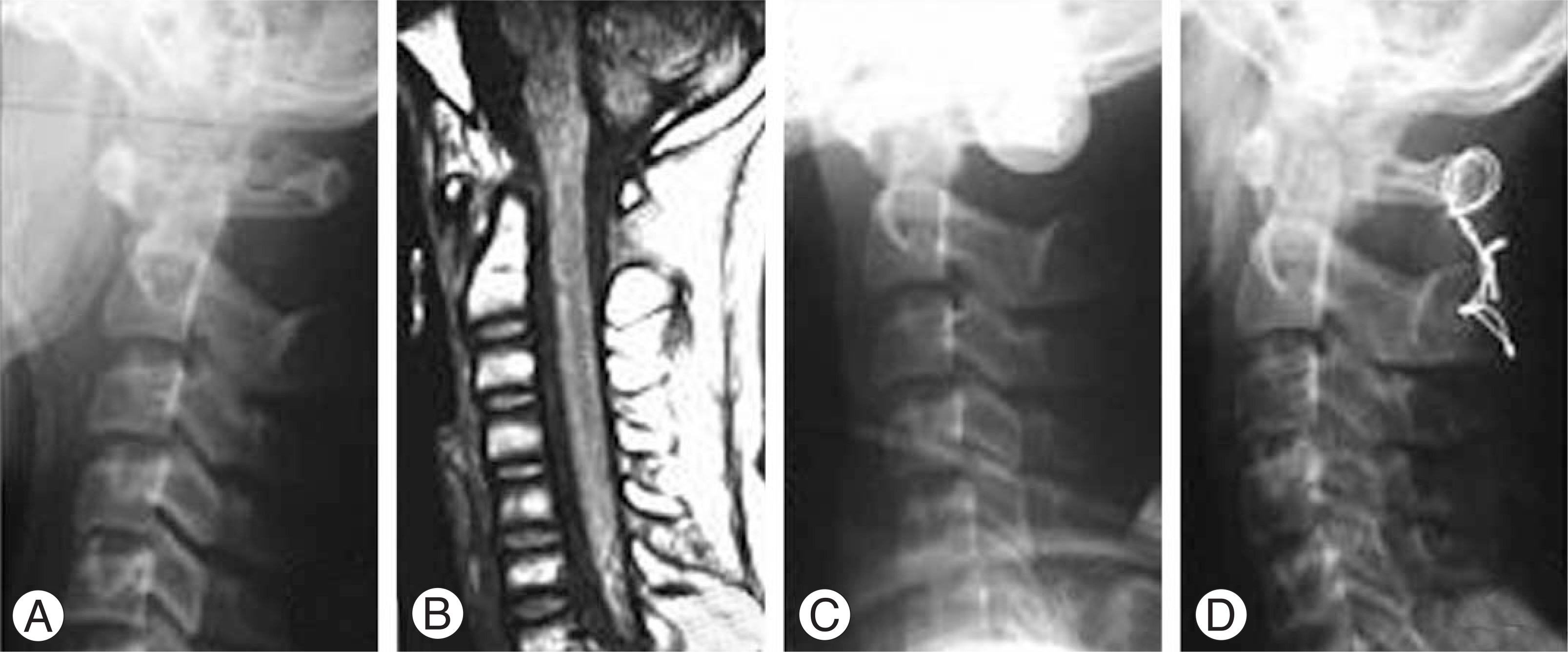
Fig. 1. 17 year-old man sustainted a type IIb occitocervical dislocation in motor vehicle accident. (A) Initial lateral plain radiograph shows isolated C1-2 dislocation with 11mm of vertical C1-2 gap and 10mm of ADI. (B) Noncontrast T1-weighted sagittal MRI shows vertical migration and anterior displacement of atlas. (C) He was immobilized in halo vest and posterior arthrodesis between C1-2. (D) One year after operation, he had satisfactory alignment and solid fusion.

Fig. 2. (A) Lateral spine radiograph showing the anterior displacement of C4 on C5 body. (B)Anteroposterior, open-mouth radiograph showing asymmetric interval between odontoid process and lateral mass of atlas. (C) Axial image of CT showing avulsion fracture of lateral mass of atlas at the attached site of transverse alar ligament. (D, E) Treated in halo vest immobilization for 3 months and anerior interbody fusion at C4-5, 6months after completing treatment, flexion-extension radiographs were done and showed restoration of stability

Fig. 3. (A) Lateral spine radiograph shows anteriorly displaced odontoid fracture. (B) Coronal CT scan demonstrates the fracture line extended to C2 body. (C) Treated in halo vest immobilization for 3 months. (D, E) Lateral radiograph and CT scan show complete healing of odontoid in anatomical position.

Fig. 4. (A) Lateral spine radiograph shows anterior displaced type II odontoid fracture. (B) Reduction was achieved using halo traction and was fixed with one screw. (C) At 4 months, the fracture appeared healing.
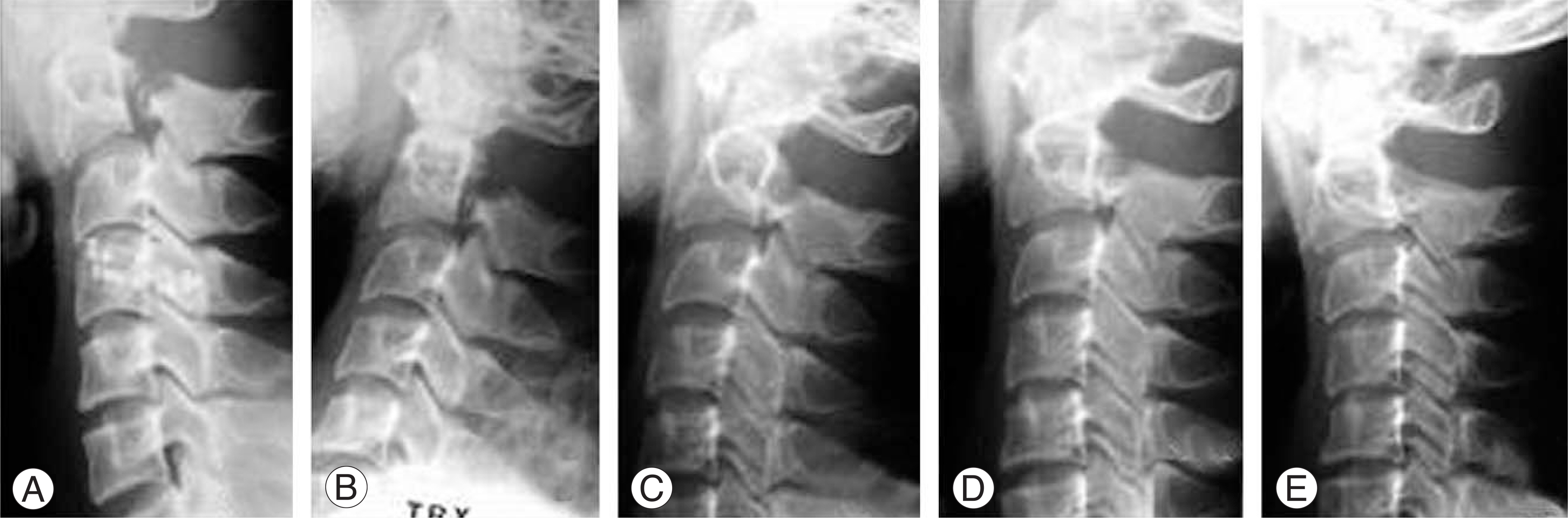
Fig. 5. (A) This 38-year-old man sustained a type II traumatic spondylolisthesis of axis in motor vehicle accident. (B) Reduction was achieved using halo traction. (C) He had halo traction and treated in halo vest immobilization for 3 months. (D, E) One year after completing treatment, flexion-extension roentgenograms were done and showed restoration of stability.

Fig. 6. (A) The patient sustained type IIA traumatic spondylolisthesis of the axis. (B) Transpedicular fixation was achieved, allowing immediate mobilization in a collar. (C, D) Anteroposterior, open-mouth radiograph showing orientation of the screws.
Reference
-
01). Clayman DA., Sykes CH., Vines FS. Occipital condyle fractures: clinical presentation and radiologic detection. Am J Neuroradiol. 1994. 15:1309–1315.02). Anderson PA., Montesano PX. Morphology and treatment of occipital condyle fractures. Spine. 1988. 13:731–736.
Article03). Hanson JA., Deliganis AV., Baxter AB, et al. Radiologic and clinical spectrum of occipital condyle fractures: retrospective review of 107 consecutive fractures in 95 patients. AJR Am J Roentgenol. 2002. 178:1261–1268.04). Bellabarba C., Mirza SK., West GA, et al. Diagnosis and treatment of craniocervical dislocation in a series of 17 consecutive survivors during an 8-year period. J Neurosurg. 2006. 4:429–440.
Article05). Fujimura Y., Nishi Y., Chiba K., Kobayashi K. Prognosis of neurological deficits associated with upper cervical spine injuries. Paraplegia. 1995. 33:195–202.
Article06). Dickman CA., Hadley MN., Pappas CT., Sonntag VK., Geisler FH. Cruciate paralysis: a clinical and radiographic analysis of injuries to the cervicomedullary junction. J Neurosurg. 1990. 73:850–858.
Article07). Matava MJ., Whitesides TE Jr., Davis PC. Traumatic atlantooccipital dislocation with survival. Serial computerized tomography as an aid to diagnosis and reduction: a report of three cases. Spine. 1993. 18:1897–1903.08). Eismont FJ., Bohlman HH. Posterior atlanto-occipital dislocation with fractures of the atlas and odontoid process. J Bone Joint Surg Am. 1978. 60:397–399.
Article09). Dickman CA., Papadopoulos SM., Sonntag VK, et al. raumatic occipitoatlantal dislocations. J Spinal Disord. 1993. 6:300–313.10). Montane I., Eismont FJ., Green BA. Traumatic occipitoatlantal dislocation. Spine. 1991. 16:112–116.
Article11). Van Den Bout AH., Commisse GF. Traumatic atlantooccipital dislocation. Spine. 1986. 11:174–176.
Article12). Traynelis VC., Marano GD., Dunker RO., Kaufman HH. Traumatic atlanto-occipital dislocation. Case report. J Neurosurg. 1986. 65:863–870.13). Sun PP., Poffenbarger GJ., Durham S., Zimmerman RA. Spectrum of occipitoatlantoaxial injury in young children. J Neurosurg. 2000. 93:28–30.
Article14). Floman Y., Kaplan L., Elidan J., Umansky F. Transverse ligament rupture and atlantoaxial subluxation in children. J Bone Joint Surg Br. 1991. 73:640–643.
Article15). Blackmore CC., Ramsey SD., Mann FA., Deyo RA. Cervical spine screening with CT in trauma patients: a cost-effectiveness analysis. Radiology. 1999. 212:117–125.
Article16). Wasserberg J., Bartlett RJ. Occipital condyle fractures diagnosed by high-definition CT and coronal reconstructions. Neuroradiology. 1995. 37:370–373.
Article17). Grob D. Transarticular screw fixation for atlanto-occipital dislocation. Spine. 2001. 26:703–707.
Article18). Jeanneret B., Magerl F. Primary posterior fusion C1/2 in odontoid fractures: indications, technique, and results of transarticular screw fixation. J Spinal Disord. 1992. 5:464–475.19). Harms J., Melcher RP. Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine. 2001. 26:2467–2471.
Article20). Sherk HH. Lesions of the atlas and axis. Clin Orthop Relat Res. 1975. 109:33–41.
Article21). Wigren A., Sweden U., Amici F Jr. Traumatic atlantoaxial dislocation without neurological disorder. A case report. J Bone Joint Surg Am. 1973. 55:642–644.22). Fielding JW., Cochran GB., Lawsing JF 3rd., Hohl M. Tears of the transverse ligament of the atlas. A clinical and biomechanical study. J Bone Joint Surg Am. 1974. 56:1683–1601.23). Levine AM., Edwards CC. Traumatic lesions of the occipitoatlantoaxial complex. Clin Orthop Relat Res. 1989. 239:53–68.
Article24). Pennecot GF., Leonard P., Peyrot Des Gachons S., Hardy JR., Pouliquen JC. Traumatic ligamentous instability of the cervical spine in children. Pediatr Orthop. 1984. 4:339–345.
Article25). O'Brien JJ., Butterfield WL., Gossling HR. Jefferson fracture with disruption of the transverse ligament. A case report. Clin Orthop Relat Res. 1977. 126:135–138.26). Spence KF Jr., Decker S., Sell KW. Bursting atlantal fracture associated with rupture of the transverse ligament. J Bone Joint Surg Am. 1970. 52:543–549.
Article27). Fielding JW., Hawkins RJ., Ratzan SA. Spine fusion for atlanto-axial instability. J Bone Joint Surg Am. 1976. 58:400–407.
Article28). Deliganis AV., Baxter AB., Hanson JA, et al. Radiologic spectrum of craniocervical distraction injuries. Radiolo-graphics. 2000. 20:237–250.
Article29). Dickman CA., Greene KA., Sonntag VK. Injuries involving the transverse atlantal ligament: classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery. 1996. 38:44–50.
Article30). Tokuhashi Y., Matsuzaki H., Shirasaki Y., Tateishi T. C1-C2 intra-articular screw fixation for atlantoaxial posterior stabilization. Spine. 2000. 25:337–341.
Article31). Xu R., Ebraheim NA., Misson JR., Yeasting RA. The reliability of the lateral radiograph in determination of the optimal transarticular C1-C2 screw length. Spine. 1998. 23:2190–2194.
Article32). Levin AM., Edwards CC. Fractures of the atlas. J Bone Joint Surg Am. 1991. 73:680–691.33). Kontautas E., Ambrozaitis KV., Kalesinskas RJ., Spakauskas B. Management of acute traumatic atlas fractures. J Spinal Disord Tech. 2005. 18:402–405.
Article34). Schatzker J., Rorabeck CH., Waddell JP. Fractures of the dens (odontoid process). An analysis of thirty-seven cases. J Bone Joint Surg Br. 1971. 53:392–405.35). Apfelbaum RI., Lonser RR., Veres R., Casey A. Direct anterior screw fixation for recent and remote odontoid fractures. J Neurosurg. 2000. 93:227–236.
Article36). Borne GM., Bedou GL., Pinaudeau M., Cristino G., Hus-sein A. Odontoid process fracture osteosynthesis with a direct screw fixation technique in nine consecutive cases. J Neurosurg. 1988. 68:223–226.37). Fujii E., Kobayashi K., Hirabayashi K. Treatment in fractures of the odontoid process. Spine. 1988. 13:604–609.
Article38). Bucholz RW., Burkhead WZ., Graham W., Petty C. Occult cervical spine injuries in fatal traffic accidents. J Trauma. 1979. 19:768–771.
Article39). Huelke DF., O'Day J., Mendelsohn RA. Cervical injuries suffered in automobile crashes. J Neurosurg. 1981. 54:316–322.
Article40). Anderson LD., D'Alonzo RT. Fractures of the odontoid process of the axis. J Bone Joint Surg Am. 1974. 56:1663–1674.
Article41). Apuzzo ML., Heiden JS., Weiss MH., Ackerson TT., Harvey JP., Kurze T. Acute fractures of the odontoid process. An analysis of 45 cases. J Neurosurg. 1978. 48:85–91.42). Wang GJ., Mabie KN., Whitehill R., Stamp WG. The nonsurgical management of odontoid fractures in adults. Spine. 1984. 9:229–230.
Article43). Clark CR., White AA III. Fractures of the dens. A multi-center study. J Bone Joint Surg. 1985. 67:1340–1348.
Article44). Greene KA., Dickman CA., Marciano FF., Drabier JB., Hadley MN., Sonntag VK. Acute axis fractures. Analysis of management and outcome in 340 consecutive cases. Spine. 1997. 22:1843–1853.45). Lennarson PJ., Mostafavi H., Traynelis VC., Walters BC. Management of type II dens fractures: a case-control study. Spine. 2000. 25:1234–1237.46). Park HJ., Rah JH., Lee YS. Treatment for odontoid fractures using anterior screw fixation. J Kor Spine Surg. 1994. 1:11–18.47). Montesano PX., Anderson PA., Schlehr F., Thalgott JS., Lowrey G. Odontoid fractures treated by anterior odontoid screw fixation. Spine. 1991. 16(Suppl):33–37.
Article48). Francis WR., Fielding JW., Hawkins RJ., Pepin J., Hensinger R. Traumatic spondylolisthesis of the axis. J Bone Joint Surg Br. 1981. 63:313–318.
Article49). Levine AM., Edwards CC. The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am. 1985. 67:217–226.
Article50). Hadley MN., Dickman CA., Browner CM., Sonntag VK. Acute axis fractures: a review of 229 cases. J Neurosurg. 1989. 71:642–647.
Article51). Effendi B., Roy D., Cornish B., Dussault RG., Laurin CA. Fractures of the ring of the axis. A classification based on the analysis of 131 cases. J Bone Joint Surg Br. 1981. 63:319–327.
Article52). Dussault RG., Effendi B., Roy D., Cornish B., Laurin CA. Locked facets with fracture of the neural arch of the axis. Spine. 1983. 8:365–367.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pattern of Cervical Spine Injury in Patients with a Facial Fracture
- Cervical Deformity Arising From Upper Thoracic Malalignment
- Clinical Analysis of Upper Cervical Spine Injuriesur
- Missed Traumatic Cervical Spine Injury
- Delayed or Missed Diagnosis of Cervical Instability after Traumatic Injury: Usefulness of Dynamic Flexion and Extension Radiographs
