J Korean Soc Spine Surg.
2009 Jun;16(2):104-111. 10.4184/jkss.2009.16.2.104.
Radiological and Clinical Comparison of 1 Cage versus 2 Cages for Posterior Lumbar Interbody Fusion with PEEK Cage and Local Bone Graft
- Affiliations
-
- 1Department of Orthopedic Surgury, Gil Medical Center, Gachon University of Medicine and Science, Korea. shinwj72@gilhospital.com
- KMID: 2209604
- DOI: http://doi.org/10.4184/jkss.2009.16.2.104
Abstract
-
STUDY DESIGN: This is a retrospective study.
OBJECTIVES
We wanted to compare and evaluate the results of using one cage and two cages with local bone grafting for each segment when performing posterior lumbar interbody fusion (PLIF). Summary of Literature Review: Some authors have reported that unilateral one-caged PLIF with local bone grafting and posterior instrumentation was no difference from bilateral two-caged PLIF regard to the fusion rates and the radiologic or clinical results.
MATERIALS AND METHODS
From March 2005 to February 2006, PLIF was performed on 36 patients who had lumbar degenerative disease. They were categorized as the cases for which one cage was used for a segment and the cases for which 2 cages were used for a segment. The clinical and radiological results in each group were compared.
RESULTS
There was complete union in 11 segments with using one cage (55%), complete union in 12 segments using two cages (77%) and incomplete unions in 9 segments with using one cage (45%) and incomplete union in 4 segments with using 2 cages (25%), and there wasn't any case of nonunion (p>0.05). The postoperative changes of the intervertebral disc space were a 2.0 mm increase with using one cage and a 2.2 mm increase with using two cages, yet these values decreased by 0.4 mm and 0.3 mm, respectively, on the last follow-up. The mean operation time was 89 minutes for one segment with one cage and 105 minutes for one segment with two cages. The blood loss was a mean of 602 ml with one cage and 802 ml with two cages (p<0.05). There was no significant difference between the one cage group and the two cages group for the Kirkadly-Willis criteria.
CONCLUSION
Posterior decompression and PLIF with one PEEK cage for treating degenerative lumbar disease was more effective for the operation time and the amount of blood loss than that with two cages, but the fusion rate, the alteration of the intervertebral disc space, the improvement of pain and the clinical results were no different. However, these results are from short term follow up, so continuous follow up will be necessary in the future for assessing the long term prognosis.
MeSH Terms
Figure
-
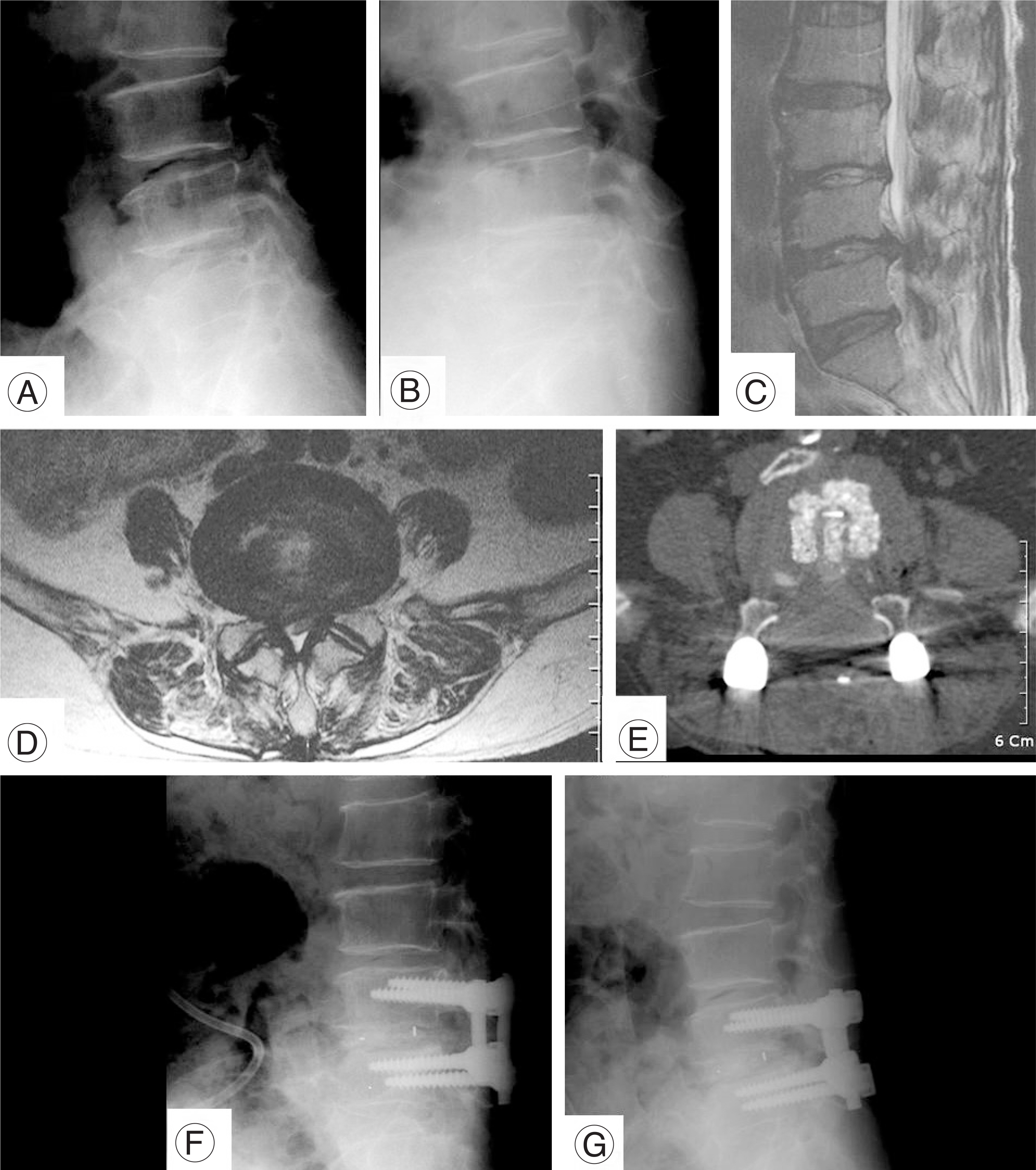
Fig. 1. The Lateral flexion and extension radiographes show L45 angular instability (A, B) and sagittal and axial T2 WI of MRI show the stenotic lesion (C, D). Postoperative CT shows the central located cage and bone graft around the cage (E). After 1 year, the postoperative lateral flexion and extension radiographes show the no instability (F, G).

Fig. 2. The figures show the straight ring and angled curettes (A), pushers (B) and bone funnels (C)
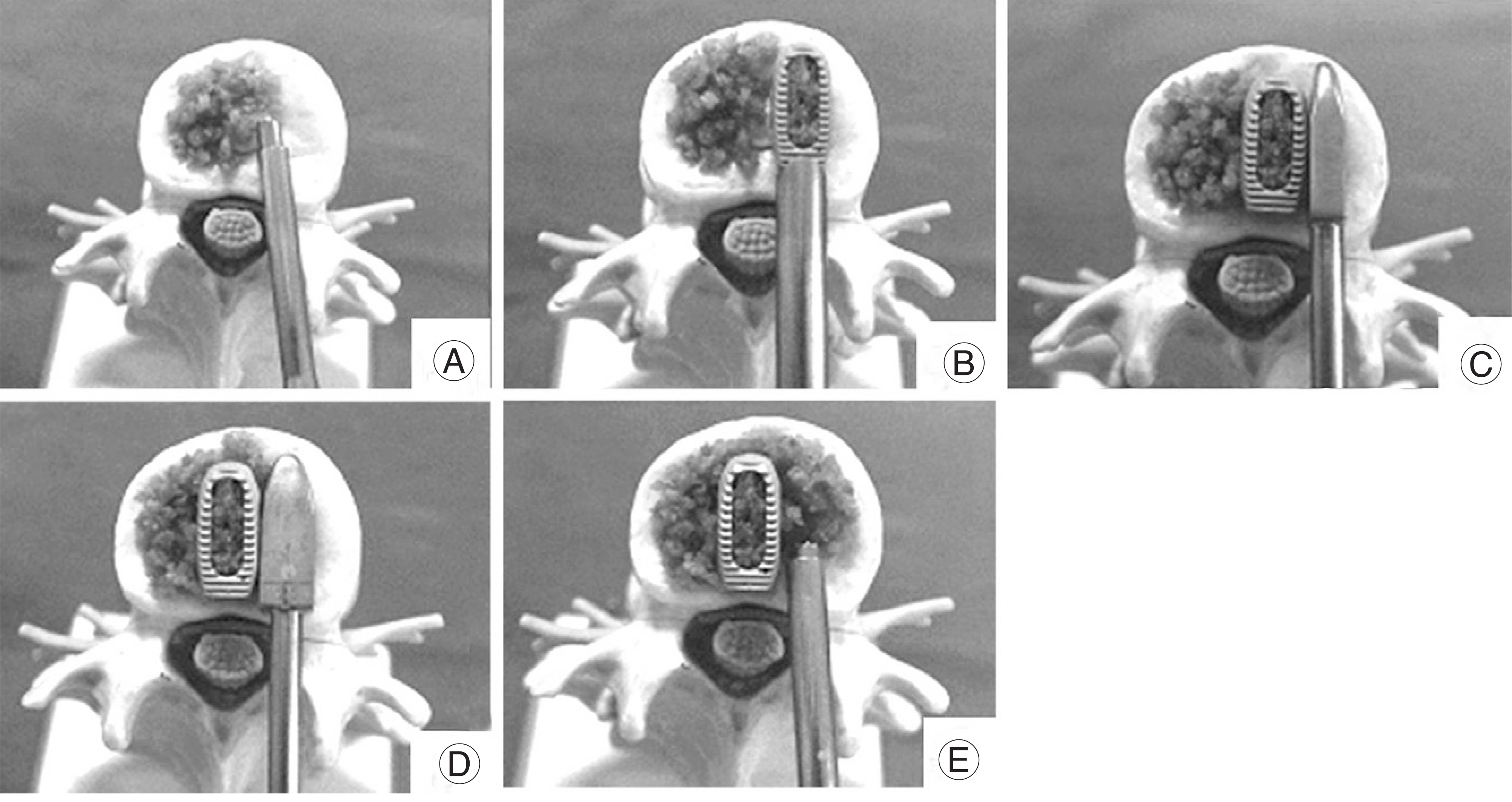
Fig. 3. The figures are showing the sequence of one PEEK cage insertion and bone graft. (A~E)
Reference
-
1). Cloward RB. The treatment of ruptured intervertebral disc by vertebral body fusion. Indication, operative techniques and after care. J Neurosurg. 1953; 10:154–168.2). Bagby GW. Arthrodesis by the distraction-compression method using a stainless steel implant. Orthopedics. 1988; 11:931–934.
Article3). Lee JC, Cha JS, Song HY, Kim YL, Shin BJ. Posterior lumbar interbody fusion using titanium cages and morselized local bone autograft. J of Korean Soc Spine Surg. 2006; 13:284–291.
Article4). Guy RF, John ST, Arvo N, John WB. Is one cage enough in posterior lumbar interbody fusion: A comparison of unilateral single cage interbody fusion to bilateral cages. J Spinal Disord Tech. 2007; 20:60–65.5). Lee CS, Chung SS, Chung KH. Comparison of unilateral and bilateral approaches for posterior lumbar interbody fusion. J of Korean Orthop Assoc. 2004; 39:642–647.
Article6). Harms J, Jeszenszky D, Stolze D. True spondylolisthesis reduction and more segmental fusion in spondylolisthesis. (In:. Bridwell KH, DeWald RL, editors. eds.Textbook of Spinal Surgery. Philadelphia: Lippincott-Raven;p. 1337–1347. 1997.7). Closkey RF, Parsons JR, Lee CK, Blacksin MF, Zimmerman MC. Mechanics of interbody spinal fusion. Analysis of critical bone graft area. Spine. 1993; 18:1011–1015.8). Ames CP, Acosta FL Jr, Chi J, et al. .:. Biomechanical comparison of posterior lumbar interbody fusion and transforaminal lumbar interbody fusion performed at 1 and 2 levels. Spine. 2005; 30:562–566.
Article9). Kettler A, Schmoelz W, Kast E, Gottwald M, Claes L, Wilke HJ. .:. In vitro stabilizing effect of a transforaminal compared with two posterior lumbar interbody fusion cages. Spine. 2005; 30:665–670.
Article10). Molinari RW, Sloboda J, Johnstone FL. .:. Are 2 cages needed with instrumented PLIF? A comparison of 1 versus 2 interbody cages in a military population. Am J Orthop. 2003; 32:337–343.11). Harris BM, Hilibrand AS, Savas PE, et al. .:. Transforaminal lumbar interbody fusion: the effect of various instrumentation techniques on the flexibility of the lumbar spine. Spine. 2004; 29:65–70.12). Wang ST, Goel VK, Fu CY, et al. .:. Posterior instrumentation reduces differences in spine stability as a result of different cage orientations: an in vitro study. Spine. 2005; 30:62–67.13). Javernick MA, Kuklo TR, Polly DW Jr. .:. Transforaminal lumbar interbody fusion: unilateral versus bilateral disk removal-an in vivo study. Am J Orthop. 2003; 32:344–348.14). David S, Thomas A. Mater techniques in orthopeadic surgery. The spine. 2nd ed.Lippincott: Williams & Wilkins Co;p. 307. 2004.15). Prolo DJ, Oklund SA, Butcher M. Toward uniformity in evaluating results of lumbar spine operations. A paradigm applied to posterior lumbar interbody fusions. Spine. 1986; 11:601–606.16). Serhan H. Presentation of mechanical testing of the Brantigan cage: In the Orthopaedics and Rehabilitation Devices Advisory Panel Meeting of the Department of Health and Human Services, Public Health Service, Food and Drug Administration. Maryland: Bethesda;1997.17). Humphreys SC, Hodges SD, Patwardhan AG, Eck JC, Murphy RB, Covington LA. .:. Comparison of posterior and transforaminal approaches to lumbar interbody fusion. Spine. 2001; 26:567–571.
Article18). Vadapalli S, Khandha A, Goel VK, et al. .:. PEEK spacers promote better bone graft fusion and lesser subsidence across a spinal segment as compared to titanium spacers-A biomechanical rationale. Paper presented at: 51st Annual Meeting of the Orthopaedic Research Society; February 20-23. 2005.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Polyetheretherketone Versus Titanium Cages for Posterior Lumbar Interbody Fusion: Meta-Analysis and Review of the Literature
- Posterior Lumbar Interbody Fusion Using New Hydroxyapatite Block: Comparison with Metal and PEEK Cages
- Posterior Lumbar Interbody Fusion Using a Unilateral Single Cage and a Local Morselized Bone Graft in the Degenerative Lumbar Spine
- A Retrospective Comparative Study to Evaluate the Clinical Efficacy Using a Bioactive Glass Ceramic Spacer in Posterior Lumbar Interbody Fusion
- Biportal Endoscopic Transforaminal Lumbar Interbody Fusion Using Double Cages: Surgical Techniques and Treatment Outcomes
