Image Quality and Radiation Exposure in Coronary CT Angiography According to Tube Voltage and Body Mass Index
- Affiliations
-
- 1Department of Radiology, Korea University Guro Hospital, Korea University College of Medicine, Korea.
- 2Department of Radiology, Ewha Womans University MokDong Hospital, Korea. yookkim@ewha.ac.kr
- KMID: 2208991
- DOI: http://doi.org/10.3348/jksr.2010.62.1.29
Abstract
- PURPOSE
To investigate the image quality and radiation dose of a coronary CT angiography (CCTA) according to tube voltage and body mass index (BMI).
MATERIALS AND METHODS
This study included 139 patients who underwent CCTA using a retrospective electrocardiography- gating technique. A total of 48 patients (BMI <2 5, group A) were examined with 100 kVp, 45 patients (BMI > 25, group B) with 120 kVp, and 46 patients (BMI < 25, group C) with 120 kVp. Attenuation and image noise of the aorta and coronary arteries was measured. Moreover, the image quality of 9 coronary segments was graded on a scale of 1-5, where grade 4 or 5 was considered to be diagnostic. Image quality parameters and radiation dose were compared using a t-test or Chi-squared test.
RESULTS
Vessel attenuation in group A was significantly higher than in groups B or C (group A, 592 +/- 85 HU; group B, 437 +/- 46 HU; group C, 469 +/- 62 HU, p<0.001). Image noise was similar in group A and group B (23 +/- 5 HU versus 22 +/- 6 HU, p=0.427), but significantly higher in group A compared to group C (23 +/- 5 HU versus 17 +/- 4 HU, p<0.001). A significant difference was observed in the signal-to-noise ratio between the three groups (group A, 24 +/- 6; group B, 19 +/- 3; group C, 27 +/- 5: p<0.05). Moreover, the contrast-to-noise ratio was significantly higher in group A than group B (group A 18 +/- 5 versus group B 14 +/- 3, p < 0.001) but not significantly different between group A and group C (group C 20 +/- 4, p=0.127). The percentage of coronary segments with diagnostic image quality was 97.9% in group A, 96.0% in group B, and 99.0% in group C. The mean image quality score was 4.5 +/- 0.5 in group A, 4.1 +/- 0.4 in group B, and 4.2 +/- 0,4 in group C (p<0.001). The effective radiation doses were 8.5 +/- 0.8 mSv in group A, 14.3 +/- 1.3 mSv in group B, and 14.9 +/- 1.3 mSv in group C. A 42% reduction in mean effective radiation dose in group A was observed compared with groups B and C.
CONCLUSION
In patients with BMI less than 25 and a low-dose CCTA with 100 kVp leads to a significant reduction in radiation exposure without degradation of image quality.
MeSH Terms
Figure
-
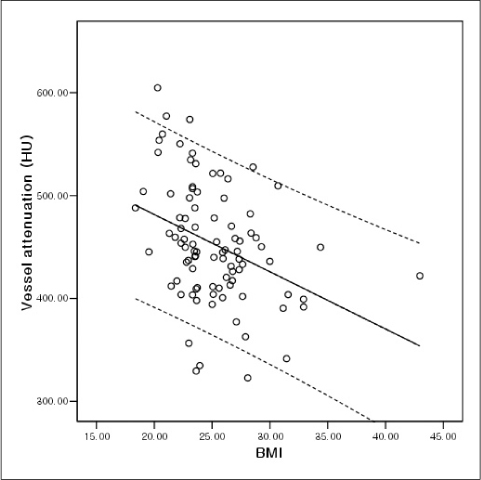
Fig. 1 Linear regression plot of mean vessel attenuation against body mass index shows significant negative dependency (r=-0.364, p<0.001). Solid line = mean; dashed lines = 95% confidence interval.
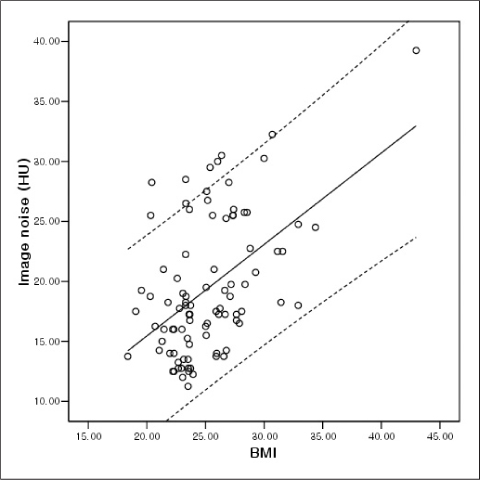
Fig. 2 Linear regression plot of image noise against body mass index shows significant positive dependency (r=0.498, p<0.001). Solid line = mean; dashed lines = 95% confidence interval.
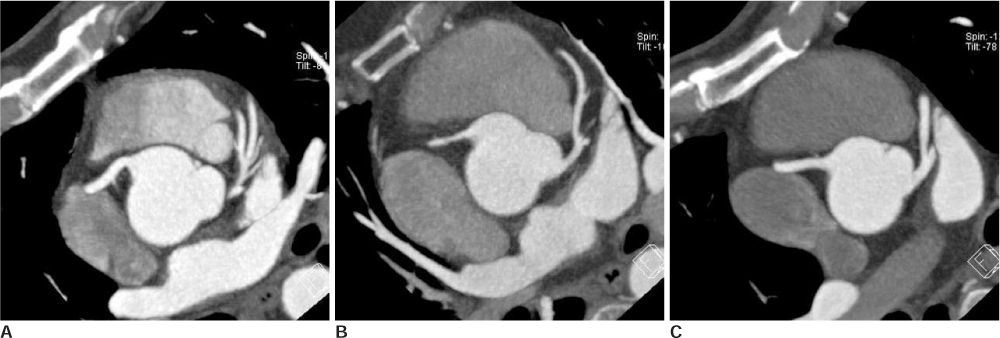
Fig. 3 A-C. CT images in representative coronary CT angiography studies of group. A. 44-year-old man from group A with BMI of 24.0 kg/m2. Axial CT image obtained at 100 kVp shows diagnostic image quality with vessel attenuation of 610 HU and image noise of 21 HU. Estimated radiation dose was 7.4 mSv. B. 56-year-old woman from group B with BMI of 27.4 kg/m2. Axial CT image obtained at 120 kVp shows diagnostic image quality with vessel attenuation of 495 HU and image noise of 28 HU. Estimated radiation dose was 12.5 mSv. C. 41-year-old man from group C with BMI of 23.5 kg/m2. Axial CT image obtained at 120 kVp shows diagnostic image quality with vessel attenuation of 518 HU and image noise of 14 HU. Estimated radiation dose was 14.6 mSv.
Reference
-
1. Mollet NR, Cademartiri F, van Mieghem CA, Runza G, McFadden EP, Baks T, et al. High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conventional coronary angiography. Circulation. 2005; 112:2318–2323.2. Leschka S, Alkadhi H, Plass A, Desbiolles L, Grünenfelder J, Marincek B, et al. Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J. 2005; 26:1482–1487.3. Husmann L, Schepis T, Scheffel H, Gaemperli O, Leschka S, Valenta I, et al. Comparison of diagnostic accuracy of 64-slice computed tomography coronary angiography in patients with low, intermediate, and high cardiovascular risk. Acad Radiol. 2008; 15:452–461.4. Hausleiter J, Meyer T, Hadamitzky M, Huber E, Zankl M, Martinoff S, et al. Radiation dose estimates from cardiac multislice computed tomography in daily practice: impact of different scanning protocols on effective dose estimates. Circulation. 2006; 113:1305–1310.5. Leschka S, Stolzmann P, Schmid FT, Scheffel H, Stinn B, Marincek B, et al. Low kilovoltage cardiac dual-source CT: attenuation, noise, and radiation dose. Eur Radiol. 2008; 18:1809–1817.6. Szucs-Farkas Z, Kurmann L, Strautz T, Patak MA, Vock P, Schindera ST. Patient exposure and image quality of low-dose pulmonary computed tomography angiography: comparison of 100-and 80-kVp protocols. Invest Radiol. 2008; 43:871–876.7. Stolzmann P, Leschka S, Scheffel H, Krauss T, Desbiolles L, Plass A, et al. Dual-source CT in step-and-shoot mode: noninvasive coronary angiography with low radiation dose. Radiology. 2008; 249:71–80.8. Alkadhi H, Stolzmann P, Scheffel H, Desbiolles L, Baümuller S, Plass A, et al. Radiation dose of cardiac dual-source CT: the effect of tailoring the protocol to patient-specific parameters. Eur J Radiol. 2008; 68:385–391.9. Tatsugami F, Husmann L, Herzog BA, Burkhard N, Valenta I, Gaemperli O, et al. Evaluation of a body mass index-adapted protocol for low-dose 64-MDCT coronary angiography with prospective ECG triggering. AJR Am J Roentgenol. 2009; 192:635–638.10. Jung B, Mahnken AH, Stargardt A, Simon J, Flohr TG, Schaller S, et al. Individually weight-adapted examination protocol in retrospectively ECG-gated MSCT of the heart. Eur Radiol. 2003; 13:2560–2566.11. Irie T, Inoue H. Individual modulation of the tube current-seconds to achieve similar levels of image noise in contrast-enhanced abdominal CT. AJR Am J Roentgenol. 2005; 184:1514–1518.12. Bae KT, Seeck BA, Hildebolt CF, Tao C, Zhu F, Kanematsu M, et al. Contrast enhancement in cardiovascular MDCT: effect of body weight, height, body surface area, body mass index, and obesity. AJR Am J Roentgenol. 2008; 190:777–784.13. Pflederer T, Rudofsky L, Ropers D, Bachmann S, Marwan M, Daniel WG, et al. Image quality in a low radiation exposure protocol for retrospectively ECG-gated coronary CT angiography. AJR Am J Roentgenol. 2009; 192:1045–1050.14. Sigal-Cinqualbre AB, Hennequin R, Abada HT, Chen X, Paul JF. Low-kilovoltage multi-detector row chest CT in adults: feasibility and effect on image quality and iodine dose. Radiology. 2004; 231:169–174.15. Nakayama Y, Awai K, Funama Y, Hatemura M, Imuta M, Nakaura T, et al. Abdominal CT with low tube voltage: preliminary observations about radiation dose, contrast enhancement, image quality, and noise. Radiology. 2005; 237:945–951.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Comparative Study of Image Quality and Radiation Dose with Changes in Tube Voltage and Current for a Digital Chest Radiography
- Evaluation of a Chest Circumference-Adapted Protocol for Low-Dose 128-Slice Coronary CT Angiography with Prospective Electrocardiogram Triggering
- Tube Voltage, DNA Double-Strand Breaks, and Image Quality in Coronary CT Angiography
- Effects of Iterative Reconstruction Algorithm, Automatic Exposure Control on Image Quality, and Radiation Dose: Phantom Experiments with Coronary CT Angiography Protocols
- Feasibility Study of Radiation Dose Reduction in Adult Female Pelvic CT Scan with Low Tube-Voltage and Adaptive Statistical Iterative Reconstruction
