J Korean Soc Radiol.
2010 Feb;62(2):119-122. 10.3348/jksr.2010.62.2.119.
Endovascular Treatment of Right Coronary-to-Bronchial Anastomosis with Bronchopulmonary Shunt Presenting as Coronary Steal Syndrome: A Case Report
- Affiliations
-
- 1Department of Radiology, Chosun University, College of Medicine, Korea.
- 2Department of Internal Medicine, Chosun University, College of Medicine, Korea. yykoh@chosun.ac.kr
- KMID: 2208948
- DOI: http://doi.org/10.3348/jksr.2010.62.2.119
Abstract
- The occurrence of an anastomosis between the coronary artery to the systemic artery is rare. However, the probability of hemodynamic changes sufficient to cause clinical symptoms is extremely low. Anastomosis of the coronary to bronchial artery can cause myocardial ischemia due to the decreased flow to the coronary arteries. The authors report a case of coronary to bronchial artery anastomosis presenting as coronary steal syndrome that was treated with transarterial microcoil embolization instead of surgical ligation.
MeSH Terms
Figure
-
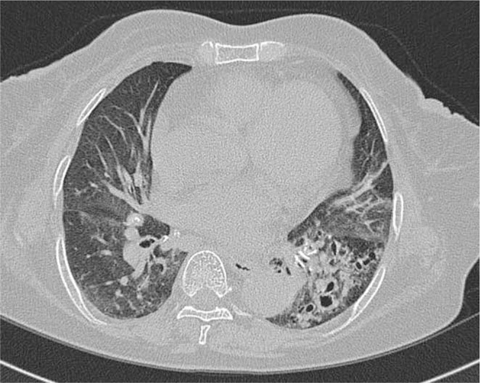
Fig. 1 Computed tomography shows bronchiectasis with peribronchial infiltration in the left lower lobe.

Fig. 2 Coronary angiography shows abnormally enlarged and tortuous artery (arrow) originated from the right coronary artery (A). On delayed phase, shunt into the pulmonary artery (black arrow) is visualized (B).
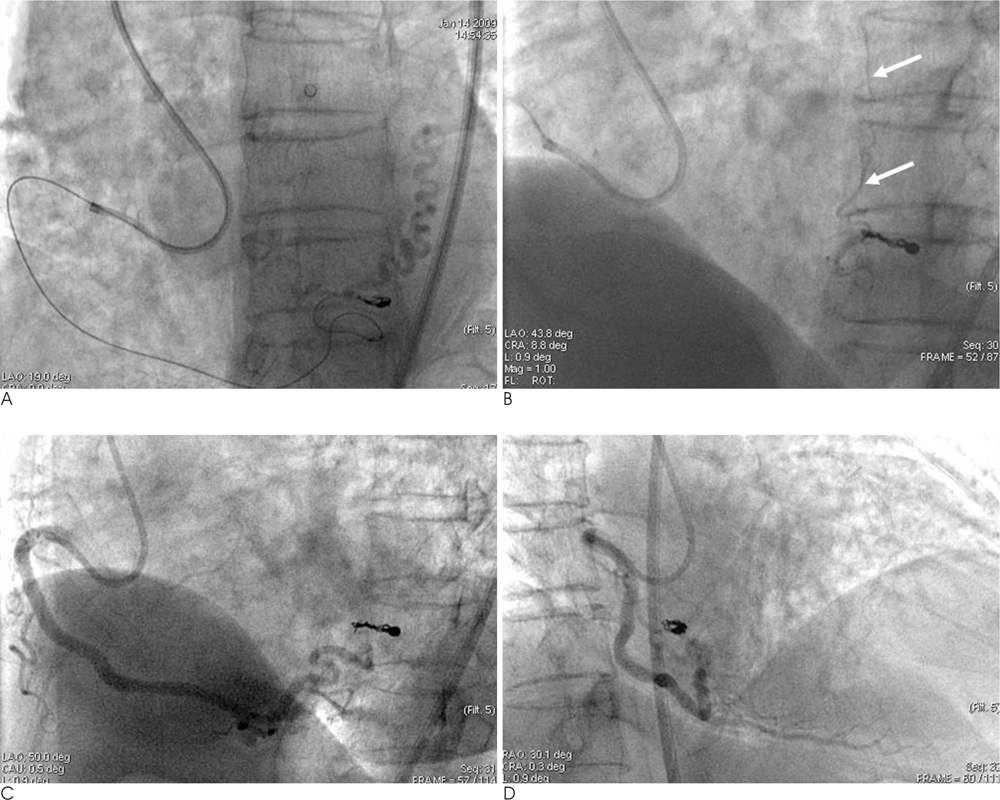
Fig. 3 Coronary-to-bronchial anastomosis was treated with transarterial microcoil embolization (A). Post-embolization angiography shows complete occlusion of anastomosis and patent branching vesseles (white arrows) (B-D).
Reference
-
1. Moberg A. Anastomoses between extracardiac vessels and coronary arteries. I. Via bronchial arteries: post-mortem angiographic study in adults and newborn infants. Acta Radiol Diagn (Stockh). 1967; 6:177–192.2. Yoon CJ, Park JH, Lee JW, Chung JW, Kim HB. Coronary to bronchial artery communication. J Korean Radiol Soc. 2000; 43:533–537.3. Green CE, Kelley MJ, Higgins CB, Bookstein JJ. Acquired coronary to bronchial artery communication: a possible cause of coronary steal. Cathet Cardiovasc Diagn. 1981; 7:191–196.4. Matsunaga N, Hayashi K, Sakamoto I, Ogawa Y, Matsuoka Y, Imamura T, et al. Coronary-to-pulmonary artery shunts via the bronchial artery: analysis of cineangiographic studies. Radiology. 1993; 186:877–882.5. Sutton SJ, Miller GA, Kerr IH, Traill TA. Coronary artery steal via large coronary artery to bronchial artery anastomosis successfully treated by operatioin. Br Heart J. 1980; 44:460–463.6. Jarry G, Bruaire JP, Commeau P, Hermida JS, Leborqne L, Auquier MA, et al. Coronary-to-bronchial artery communication: report of two patients successfully treated by embolization. Cardiovasc Intervent Radiol. 1999; 22:251–254.7. Cheon BC, Park IH, Yu JH, Chang SJ, Hong JS, Ahn KJ, et al. Enlarged coronary-bronchial artery anastomosis in cystic bronchiectasis: A case report. Korean J Med. 2007; 73:330–335.8. Aupetit JF, Gallet M, Boutarin J. Coronary-to bronchial artery anastomosis complicated with myocardial infarction. Int J Cardiol. 1988; 18:93–97.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recurrence of Coronary-Subclavian Steal Syndrome After Successful Angioplasty of Malfunctioning Arteriovenous Fistula
- Enlarged coronary-bronchial artery anastomosis in cystic bronchiectasis: A case report
- Coronary Fistula Anastomosing between Right Coronary Artery and Left Bronchial Artery Accompanied with Cystic Lung Disease
- Left Circumflex Coronary Artery Fistula Connected to the Right Bronchial Artery Associated with Bronchiectasis: Multidetector CT and Coronary Angiography Findings
- 2 Case of Coronary Artery-to-Left Ventricular Fistulae
