Recurrence of Coronary-Subclavian Steal Syndrome After Successful Angioplasty of Malfunctioning Arteriovenous Fistula
- Affiliations
-
- 1Department of Cardiology, Cardiovascular Center, Myongji Hospital, Kwandong University College of Medicine, Goyang, Korea. princette@paran.com
- KMID: 2224981
- DOI: http://doi.org/10.4070/kcj.2012.42.11.784
Abstract
- We report a case of coronary-subclavian steal syndrome, which had been masked by a malfunctioning hemodialysis access vessel and then reappeared after a successful angioplasty of multiple stenoses in the arteriovenous fistula of the left arm in a 61-year-old man. This case suggests that coronary-subclavian steal syndrome should be considered before a coronary artery bypass grafting surgery using internal mammary artery conduit is done, especially when hemodialysis using the left arm vessels is expected.
MeSH Terms
Figure
-
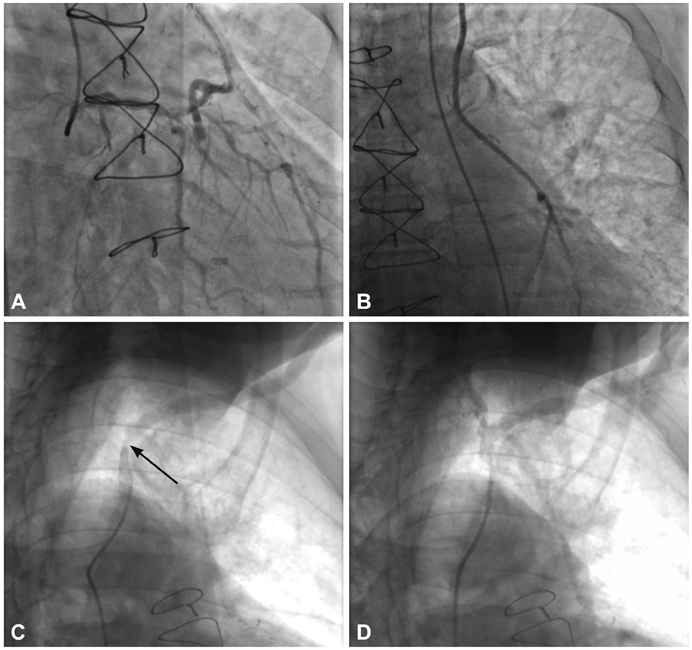
Fig. 1 Coronary angiography and left subclavian artery angioplasty 1 year prior to clinic admission. A: left coronary angiography demonstrating 'to-and-fro' flow reversal in the left internal mammary artery, suggesting coronary-subclavian steal syndrome. B: selective left internal mammary arteriography showed no significant stenosis of the left internal mammary artery graft itself while its anastomoses to native coronary arteries was demonstrated. C and D: selective left subclavian arteriography revealed a significant stenosis (80%) of the left subclavian artery (arrow) (C), which was resolved after balloon angioplasty with stenting of the left subclavian artery (D).

Fig. 2 Arteriovenous fistulogram of left arm 1 week prior to clinic admission. Multiple stenoses of the venous outflow tract (A and B), which resolved after successful balloon angioplasty (C and D), were observed.
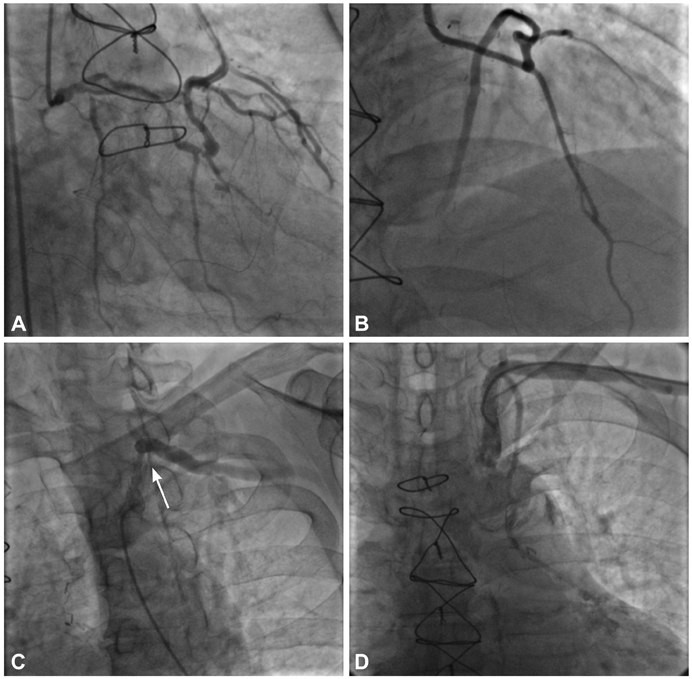
Fig. 3 Coronary angiography and left subclavian artery angioplasty on admission. A: left coronary angiography showed 'to-and-fro' flow reversal in the left internal mammary artery, suggesting coronary-subclavian steal syndrome. B: selective left internal mammary arteriography demonstrated that no significant stenosis of the left internal mammary artery graft itself was present and its anastomoses to native coronary arteries was shown. C and D: selective left subclavian arteriography showed a significant instent restenosis (80%) of the left subclavian artery (arrow) (C), which was resolved after balloon angioplasty with peripheral cutting balloon of the left subclavian artery (D).
Reference
-
1. Walker PM, Paley D, Harris KA, Thompson A, Johnston KW. What determines the symptoms associated with subclavian artery occlusive disease? J Vasc Surg. 1985. 2:154–157.2. Smith JM, Koury HI, Hafner CD, Welling RE. Subclavian steal syndrome: a review of 59 consecutive cases. J Cardiovasc Surg (Torino). 1994. 35:11–14.3. Chavan A, Mügge A, Hohmann C, Amende I, Wahlers T, Galanski M. Recurrent angina pectoris in patients with internal mammary artery to coronary artery bypass: treatment with coil embolization of unligated side branches. Radiology. 1996. 200:433–436.4. Ayres RW, Lu CT, Benzuly KH, Hill GA, Rossen JD. Transcatheter embolization of an internal mammary artery bypass graft sidebranch causing coronary steal syndrome. Cathet Cardiovasc Diagn. 1994. 31:301–303.5. Schmid C, Heublein B, Reichelt S, Borst HG. Steal phenomenon caused by a parallel branch of the internal mammary artery. Ann Thorac Surg. 1990. 50:463–464.6. Takach TJ, Reul GJ, Cooley DA, et al. Myocardial thievery: the coronary-subclavian steal syndrome. Ann Thorac Surg. 2006. 81:386–392.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of arteriovenous fistula with drainage into the coronary sinus during the percutaneous tranluminal coronary angioplasty of chronic total occlusion of circumflex coronary artery
- An Iatrogenic Coronary Arteriovenous Fistula Caused by Guidewire Trauma during Percutaneous Coronary Intervention
- A Case of Coronary Steal Syndrome Caused by a Coronary Arteriovenous Fistula: Retrograde Flow from Non-stenotic Left Anterior Descending Artery to Left Circumflex Artery
- A Rare Case of Radial Arteriovenous Fistula After Coronary Angiography
- A Case of Successful Correction of Subclavian Steal Syndrome by Percutaneus Transluminal Angioplasty with Stenting Who Found Incidentally Significant Interarm Blood Pressure Difference
