Ultrasonographic Findings of Torsed Testicular Appendages in Prepubertal Children
- Affiliations
-
- 1Department of Radiology, SMG-SNU Boramae Medical Center, Seoul, Korea. susemi513@hanmail.net
- KMID: 2208821
- DOI: http://doi.org/10.3348/jksr.2013.69.2.157
Abstract
- PURPOSE
To characterize the sonographic findings of torsed testicular appendages and to evaluate the sonographic findings in making erroneous diagnosis of epididymitis or torsion of testis in prepubertal children.
MATERIALS AND METHODS
From June 2010 to November 2012, we retrospectively analyzed the duplex sonography of fifteen children with torsion of testicular appendages. The presence or absence of the extratesticular nodule and secondary inflammatory changes were evaluated. Six patients had follow-up sonography and two patients underwent surgery.
RESULTS
Sonography demonstrated the extratesticular nodule in 13 (87%) children. Four of these 13 children were misdiagnosed as epididymitis due to imperceptions of the nodule. Out of remaining two (13%) children without the nodule, one mimicked epididymitis and the other was misdiagnosed as torsion of testis. Secondary inflammatory changes included enlarged epididymis in 14 children (93%), scrotal wall edema in 11 (73%), hydrocele in 10 (67%), and enlarged testis in 3 (20%).
CONCLUSION
Ultrasonographic findings of secondary inflammatory changes in the absence or imperception of the nodules for epididymo-testicular groove or epididymal head may suggest an erroneous diagnosis of epididymitis or torsion of testis in children with torsed testicular appendages. Meticulous evaluation for the nodule is important when differentiating the torsed testicular appendages from the two entities of prepubertal children.
MeSH Terms
Figure
-
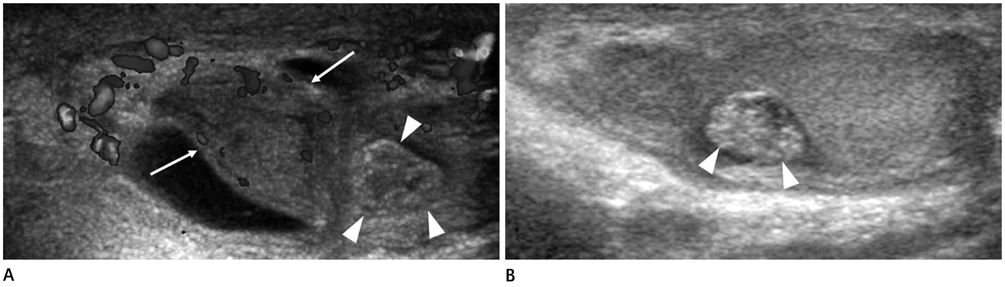
Fig. 1 Torsed testicular appendage in a 10-year-old boy who was misdiagnosed as epididymitis due to imperception of the nodule on initial ultrasonography. A. Longitudinal ultrasonography shows marked enlarged epididymal head (arrows). Mild hydrocele and scrotal wall edema are also noted. Initial operator failed to detect the mixed echoic nodule (arrowheads) and led to an erroneous diagnosis of epididymitis. B. Follow-up ultrasonography after 9 days shows the hyperechoic nodule (arrowheads) at the epididymo-testicular groove, indicating a torsed testicular appendage.
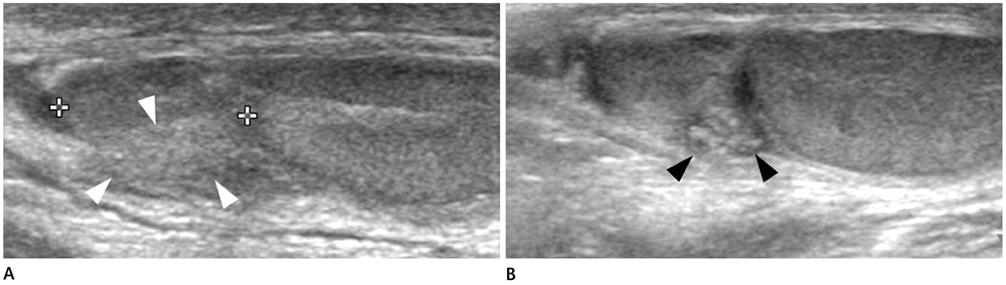
Fig. 2 Torsed testicular appendage in a 6-year-old boy who was misdiagnosed as epididymitis due to absence of the nodule on initial ultrasonography. A. Longitudinal ultrasonography shows marked enlarged epididymal head (between cursors). Initial operator misdiagnosed the isoechoic soft tissue (arrowheads) as enlarged epididymal head (between cursors) and led to an erroneous diagnosis of epididymitis. B. Follow-up ultrasonography after 5 days shows the hyperechoic nodule (black arrowheads) at the epididymo-testicular groove, indicating a torsed testicular appendage.

Fig. 3 Torsed testicular appendage in a 10-year-old boy who mimic torsion of testis. A. Transverse gray-scale (left) and color Doppler (right) ultrasonography show a whirlpool-appeared spermatic cord (arrows). B. Longitudinal ultrasonography shows the enlarged testis (between cursors) without nodule of epididymo-testicular groove, indicating torsion of testis. C. Photograph from surgery shows that the dark red nodule (arrowhead) corresponds to torsed testicular appendage. Testis (arrow) and epididymis (open arrow) are normal. Histopathologic results showed testicular appendage with signs of congestion and hemorrhage, which consisted with torsion.

Fig. 4 Torsed testicular appendage in a 11-year-old boy with pain of right scrotum for 1 day. A. Longitudinal ultrasonography shows hypoechoic nodule at epididymo-testicular groove (arrows), measuring 6.2 mm in length. B. Follow-up ultrasonography after 11 days shows interval increased size of the nodule (arrows), measuring 12.0 mm in length. Echogenicity of the nodule changed from hypoechoic to isoechoic. Progressed enlargement of epididymis (between cursors) and testis (arrowheads), and hydrocele are noted, suggesting aggravated torsion of testicular appendage with secondary inflammatory change. C. Follow-up ultrasonography after 35 days shows decreased size of nodule (arrows) and improvement of previous secondary inflammatory change. Echogenicity of the nodule changed from isoechoic to hyperechoic.
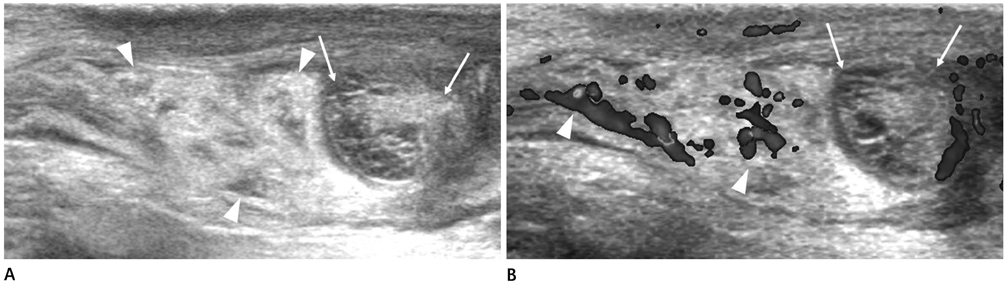
Fig. 5 Torsed testicular appendage in a 12-year-old boy with pain of right scrotum for 3 days. A. Longitudinal ultrasonography shows mixed echoic nodule at upper pole of right testis (arrows), measuring 12.5 mm in length. Prominent hyperechoic fat echogenicity (arrowheads) along the distal spermatic cord is also noted. B. Color Doppler ultrasonography shows hypervascularity along the spermatic cord (arrowheads) and avascularity of the nodule (arrows).
Reference
-
1. Strauss S, Faingold R, Manor H. Torsion of the testicular appendages: sonographic appearance. J Ultrasound Med. 1997; 16:189–192. quiz 193-194.2. Baldisserotto M, de Souza JC, Pertence AP, Dora MD. Color Doppler sonography of normal and torsed testicular appendages in children. AJR Am J Roentgenol. 2005; 184:1287–1292.3. Karmazyn B, Steinberg R, Livne P, Kornreich L, Grozovski S, Schwarz M, et al. Duplex sonographic findings in children with torsion of the testicular appendages: overlap with epididymitis and epididymoorchitis. J Pediatr Surg. 2006; 41:500–504.4. Atkinson GO Jr, Patrick LE, Ball TI Jr, Stephenson CA, Broecker BH, Woodard JR. The normal and abnormal scrotum in children: evaluation with color Doppler sonography. AJR Am J Roentgenol. 1992; 158:613–617.5. Sellars ME, Sidhu PS. Ultrasound appearances of the testicular appendages: pictorial review. Eur Radiol. 2003; 13:127–135.6. Siegel MJ. Male genital tract. In : Siegel MJ, editor. Pediatric sonography. Philadelphia: Lippincott Williams & Wilkins;2002. p. 579–624.7. Kadish HA, Bolte RG. A retrospective review of pediatric patients with epididymitis, testicular torsion, and torsion of testicular appendages. Pediatrics. 1998; 102(1 Pt 1):73–76.8. Kass EJ, Lundak B. The acute scrotum. Pediatr Clin North Am. 1997; 44:1251–1266.9. Hesser U, Rosenborg M, Gierup J, Karpe B, Nyström A, Hedenborg L. Gray-scale sonography in torsion of the testicular appendages. Pediatr Radiol. 1993; 23:529–532.10. McCombe AW, Scobie WG. Torsion of scrotal contents in children. Br J Urol. 1988; 61:148–150.11. Park SJ, Lee HK, Yi BH, Cha JG, Joh JH, Hong HS, et al. Manual reduction of torsion of an intrascrotal appendage under ultrasonographic monitoring. J Ultrasound Med. 2007; 26:293–299.12. Johnson KA, Dewbury KC. Ultrasound imaging of the appendix testis and appendix epididymis. Clin Radiol. 1996; 51:335–337.13. Park SJ, Kim HL, Yi BH. Sonography of intrascrotal appendage torsion: varying echogenicity of the torsed appendage according to the time from onset. J Ultrasound Med. 2011; 30:1391–1396.14. Frush DP, Sheldon CA. Diagnostic imaging for pediatric scrotal disorders. Radiographics. 1998; 18:969–985.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ultrasonography of intrascrotal torsed appendages: size and interval between symptom onset and the ultrasonographic examination according to echogenicity
- Early exploration of acute scrotum in children
- Overview of Pediatric Testicular Tumors in Korea
- Penile circumference and stretched penile length in prepubertal children: A retrospective, single-center pilot study
- Ultrasonographic Findings of Prepubertal Testicular Teratoma
