Infected Aortic Aneurysm Presenting as Prevertebral Abscess in Magnetic Resonance Imaging: A Case Report
- Affiliations
-
- 1Department of Internal Medicine, Jeju National University School of Medicine, Jeju, Korea. neosangtaek@naver.com
- 2Department of Radiology, Jeju National University School of Medicine, Jeju, Korea.
- KMID: 2208802
- DOI: http://doi.org/10.3348/jksr.2013.69.3.201
Abstract
- The differential diagnosis of mass-like lesions around the aorta includes saccular pseudoaneurysms and abscesses. A 69-year-old female was admitted with multiple abscesses and fluid collections in several muscles and joints. Methicillin susceptible Staphylococcus aureus was isolated from her blood and pus. Even though she was treated with repeated operations and appropriate antibiotics, her conditions worsened with persistent fever and newly developed abscesses at other sites. Serial enhanced computed tomography (CT) revealed a newly developed saccular abdominal aortic aneurysm in the retroaortic space at the celiac axis level. However, the infected aortic aneurysm mimicked a prevertebral abscess on enhanced spinal magnetic resonance imaging (MRI) due to its heterogeneous signal intensity caused by intraaneurysmal turbulent blood flow. We report to alert the pitfall in the diagnosis of saccular aortic aneurysm using spinal MRI and the importance of serial enhanced CT study in highly suspicious patients.
MeSH Terms
-
Abscess
Aged
Aneurysm, False
Aneurysm, Infected
Anti-Bacterial Agents
Aorta
Aortic Aneurysm
Aortic Aneurysm, Abdominal
Axis, Cervical Vertebra
Diagnosis, Differential
Female
Fever
Humans
Joints
Magnetic Resonance Imaging
Magnetic Resonance Spectroscopy
Magnetics
Magnets
Methicillin
Muscles
Staphylococcus aureus
Suppuration
Anti-Bacterial Agents
Methicillin
Figure
-

Fig. 1 69-year-old female with a newly developed infected aortic aneurysm (arrow) at the T12-L1 level within 4 weeks follow-up period. A. The retroarotic saccular pseudoaneurysm shows mild heterogeneous iso-signal intensity on T1-weighted MRI (arrow). The abdominal aorta shows dark signal intensity (arrowhead). B. The saccular pseudoaneurysm shows heterogeneous mixed high and dark signal intensity on T2-weighted MRI (arrow). The abdominal aorta shows dark signal intensity (arrowhead). C. Contrast-enhanced spin-echo T1-weighted MRI demonstrates the heterogeneously enhancing retroarotic saccular pseudoaneurysm (arrow) mimicking a prevertebral abscess due to intraaneurysmal turbulent blood flow and flow-related signal void. The abdominal aorta shows dark signal intensity (arrowhead) because of flow-related signal void on spin-echo MRI although the MRI is contrast-enhanced image. D. The retroaortic saccular pseudoaneurysm shows homogeneous high enhancement on contrast-enhanced CT image (arrow). The abdominal aorta also shows homogeneous high enhancement (arrowhead).
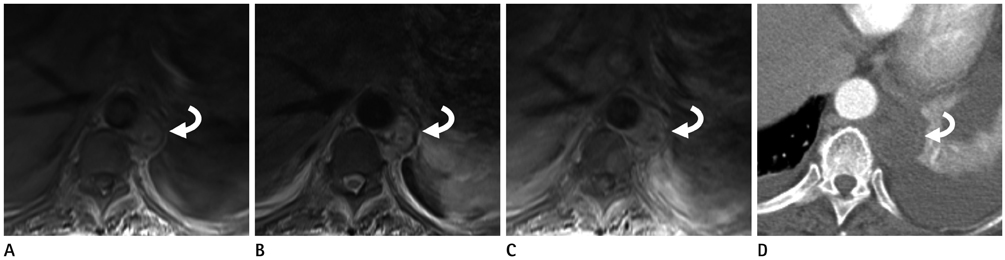
Fig. 2 69-year-old female with multiple prevertebral abscesses at the T10 level. A. The prevertebral abscess shows mild heterogeneous iso-signal intensity on T1-weighted MRI (curved arrow). B. It shows heterogeneous high signal intensity on T2-weighted MRI (curved arrow). C. It shows heterogeneous enhancement on contrast-enhanced spin-echo T1-weighted MRI (curved arrow). These MRI findings of the prevertebral abscess resembled that of the infected aortic aneurysm (Fig. 1A-C). D. However, the prevertebral abscess shows faint peripheral rim enhancement and non-enhancing central portion (curved arrow) on contrast-enhanced CT image. This CT finding was definitely different from that of the infected aortic aneurysm (Fig. 1D).
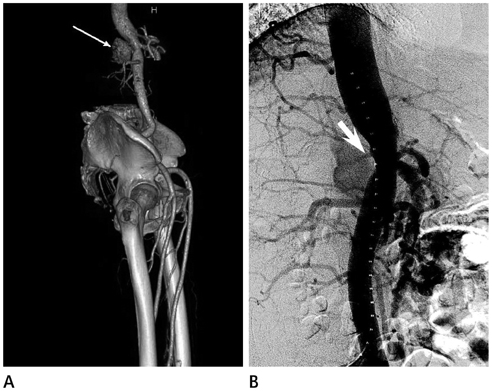
Fig. 3 69-year-old female with a newly developed infected aortic aneurysm within 4 weeks follow-up period. A. Volume rendering 3-dimentional reconstructed CT angiography shows 4 cm-sized exophytic saccular aneurysm in abdominal aorta at celiac axis level (arrow). B. Digital subtraction angiography of abdominal aorta demonstrates intraaneurysmal jet flow (arrow) causing turbulent flow in the saccular pseudoaneurysm.
Reference
-
1. Bisdas T, Teebken OE. Mycotic or infected aneurysm? Time to change the term. Eur J Vasc Endovasc Surg. 2011; 41:570. author reply 570-571.2. Oderich GS, Panneton JM, Bower TC, Cherry KJ Jr, Rowland CM, Noel AA, et al. Infected aortic aneurysms: aggressive presentation, complicated early outcome, but durable results. J Vasc Surg. 2001; 34:900–908.3. Oh SH, Lee MR, Peck KR, Kang SW, Choe YH, Kim YW, et al. A case of mycotic aneurysm of the aorta caused by Klebsiella pneumoniae accompanied by endophthalmitis. Korean J Med. 2010; 78:357–363.4. Lee WK, Mossop PJ, Little AF, Fitt GJ, Vrazas JI, Hoang JK, et al. Infected (mycotic) aneurysms: spectrum of imaging appearances and management. Radiographics. 2008; 28:1853–1868.5. Hartnell GG. Imaging of aortic aneurysms and dissection: CT and MRI. J Thorac Imaging. 2001; 16:35–46.6. Johnson JR, Ledgerwood AM, Lucas CE. Mycotic aneurysm. New concepts in therapy. Arch Surg. 1983; 118:577–582.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Ischemic Hepatitis and Pancreatic Abscess after Elective Abdominal Aortic Aneurysm Repair: A Case Report
- A Case of Infected Aortic Aneurysm Caused by Salmonella Group B
- Infected Thoracic Aortic Aneurysm Concurrent with Endophthalmitis by Candida albicans: a Case Report
- Type A Aortic Dissection with Aortocaval Fistula: Report of 1 case
- A case of infected abdominal aortic aneurysm associated with liver abscess treated by endovascular stent
