Combination Treatment of Rituximab and Plasmapheresis in Acute Cellular Rejection with Focal Segmental Glomerular Sclerosis after Renal Transplantation
- Affiliations
-
- 1Division of Nephrology, Department of Internal Medicine, Bong Seng Memorial Hospital, Busan, Korea. syhpmj@hanmail.net
- 2Department of Pathology, Yeungnam University College of Medicine, Daegu, Korea.
- KMID: 2202221
- DOI: http://doi.org/10.4285/jkstn.2010.24.1.30
Abstract
- Focal segmental glomerular sclerosis (FSGS) accounts for recurrence in 20% to 40% of the renal allografts after transplantation, and it causes graft loss in 13% to 20% of the cases. We report here on successfully treating acute cellular rejection (ACR) combined with FSGS after a kidney transplantation with a combination treatment of plasmapheresis, rituximab and steroid pulse therapy. A 53-year-old female patient whose primary kidney disease was unknown developed massive proteinuria after living donor kidney transplantation. A urine protein/creatinine ratio of 13.42 and an elevated serum creatinine level was detected on postoperative days (POD) 10 and a renal biopsy showed acute cellular rejection (Banff IIb) combined with FSGS. We started steroid pulse therapy on POD 11. She underwent 5 plasmapheresis sessions in the first 3 week after transplantation and she received one dose of rituximab (375 mg/m2) on POD 12. The proteinuria decreased below the nephrotic range at POD 20 and the serum creatinine level was normalized. Three months later, the proteinuria was at 35 mg/day with stable graft function. Rituximab and plasmapheresis is a possible option to treat FSGS combined with a relapse of proteinuria after renal transplantation.
Keyword
MeSH Terms
Figure
-
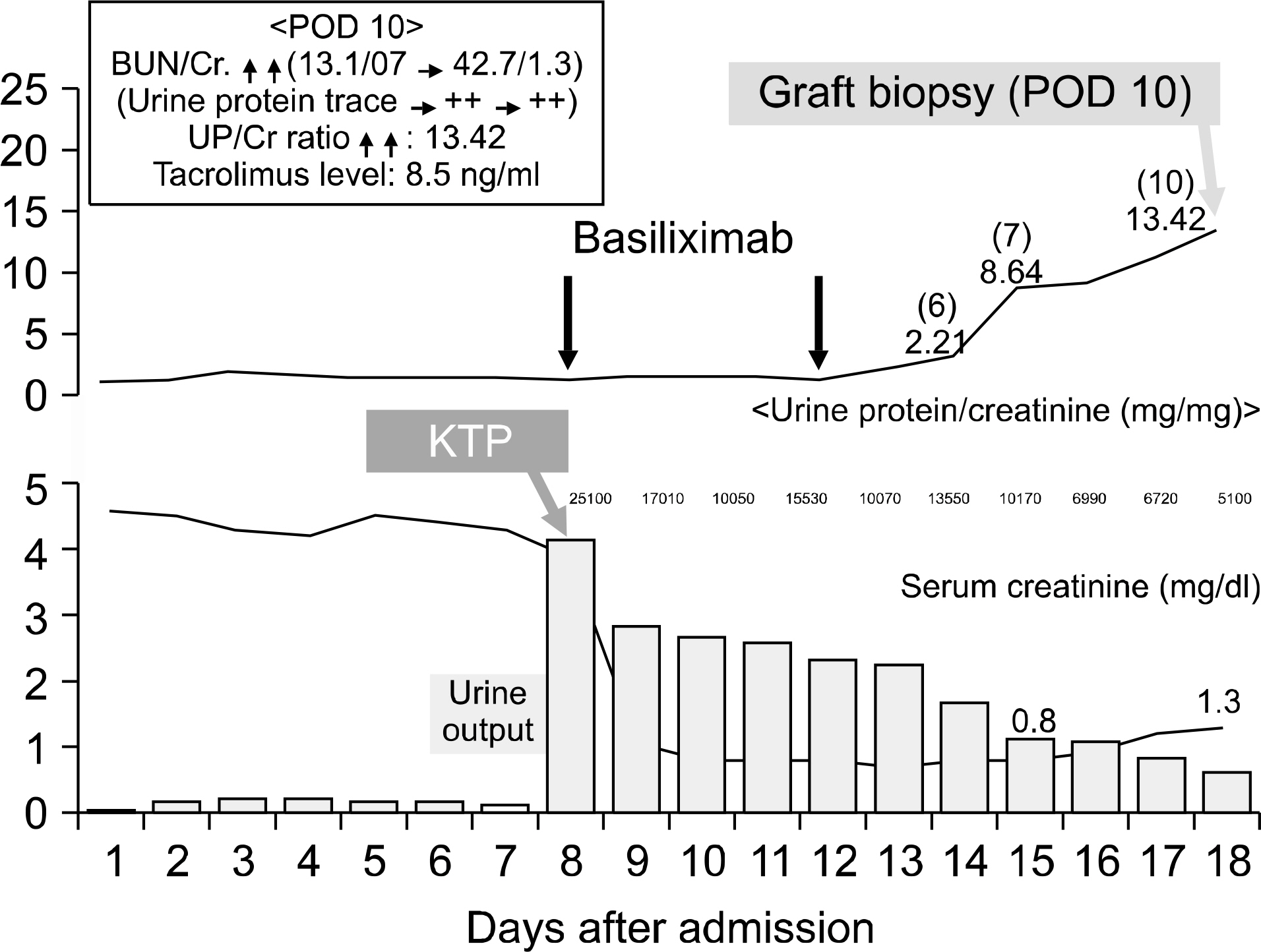
Fig. 1. Clinical course 1. Abbreviations: POD, postoperative days; BUN, blood urea nitrogen; UP, urine protein; KTP, kidney transplantation.
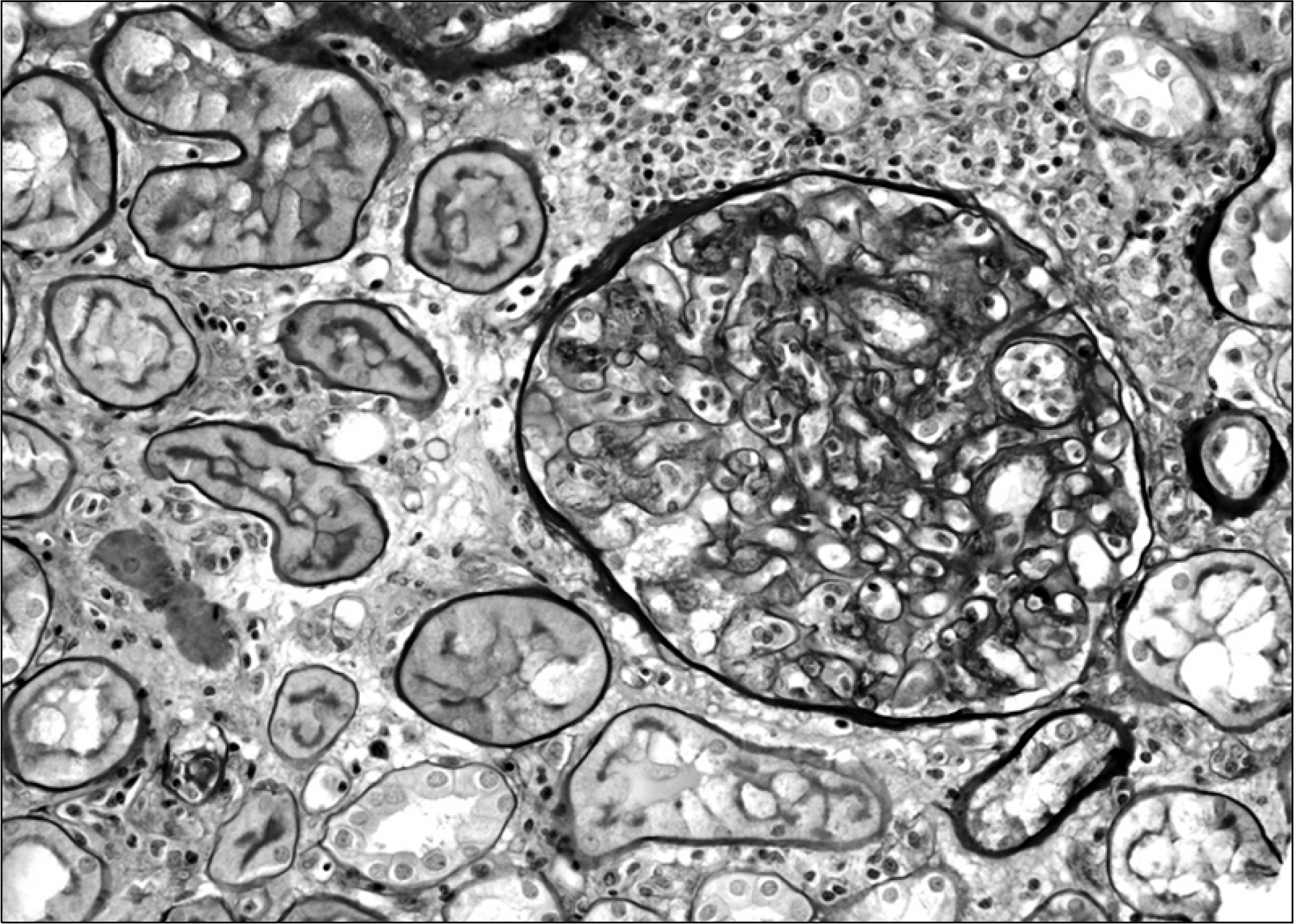
Fig. 2. Light microscopically, lymphocytic infiltration in glomerular capillary lumina is seen. Lymphocytes infiltrate along the edematous interstitium. Lymphocytic tubulitis is not present. PAS, ×200.
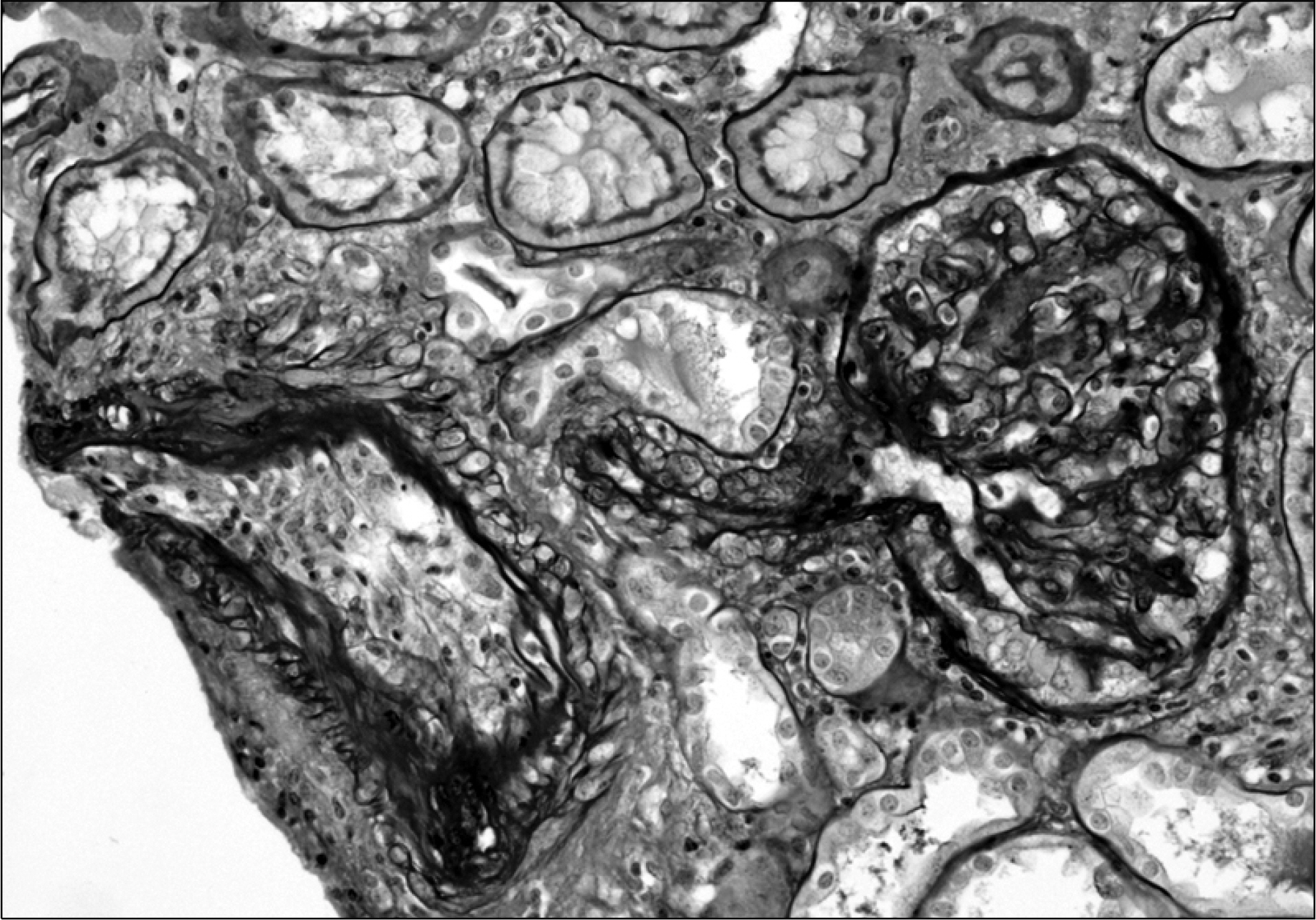
Fig. 3. On left, medium sized artery has subendothelial lymphocytic infiltration. The glomerulus shows focal mild mesangial widening. PAS, ×200.
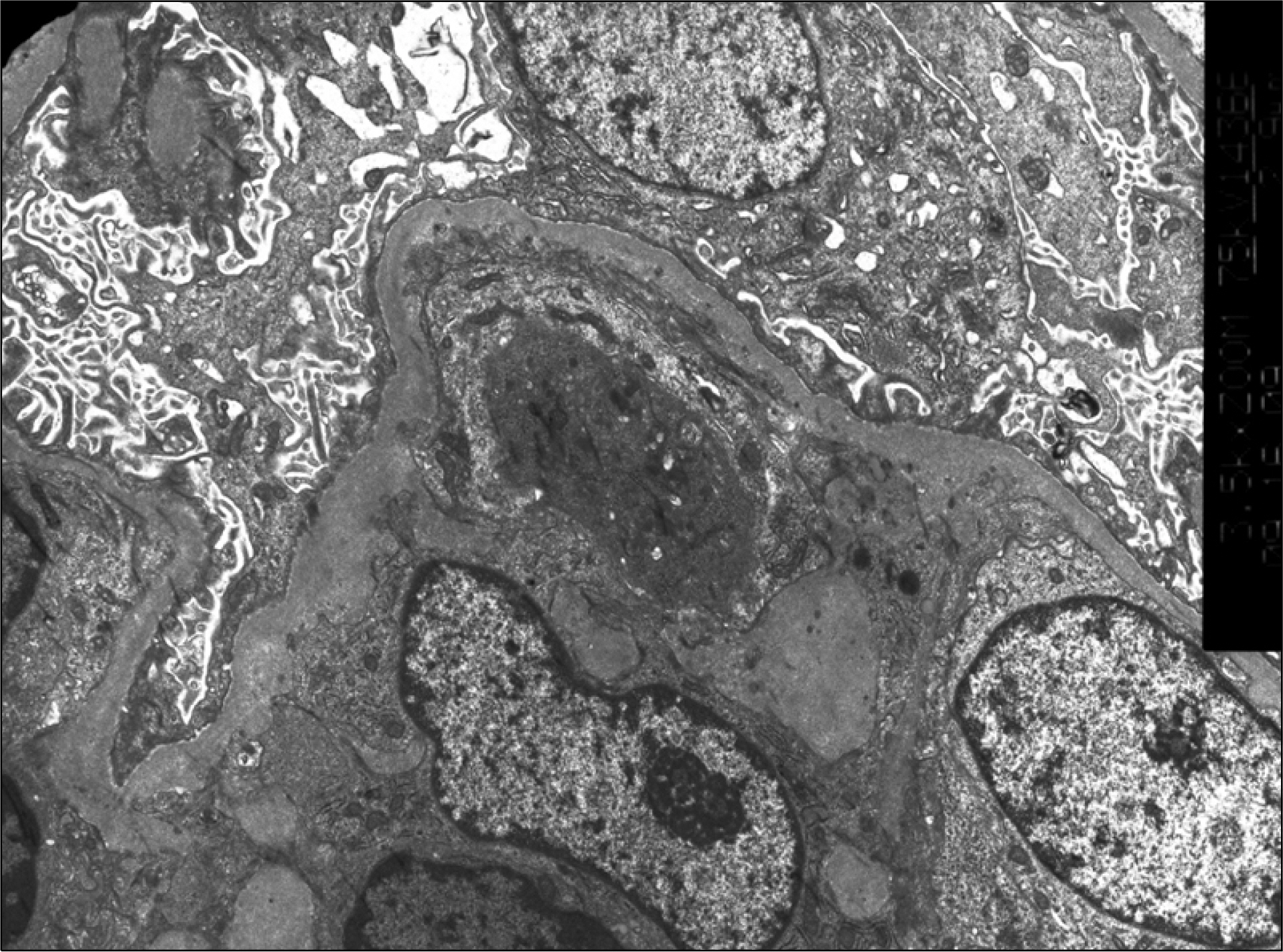
Fig. 4. Electron microscopically, most foot processes are fused with microvilli formation. ×5,000.
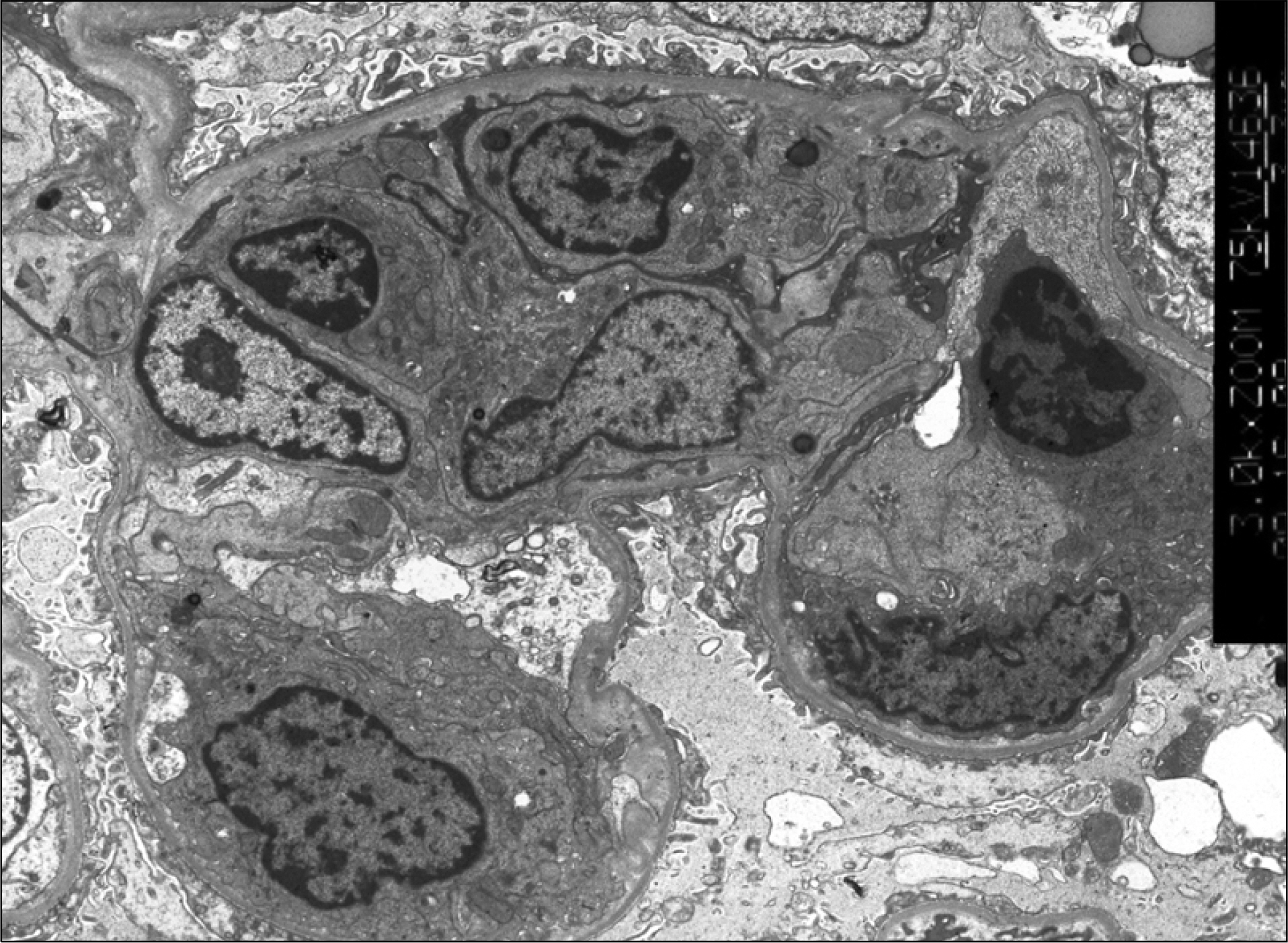
Fig. 5. Glomerular lumina are infiltrated by lymphocytes. Endothelial cells are swollen. ×500.
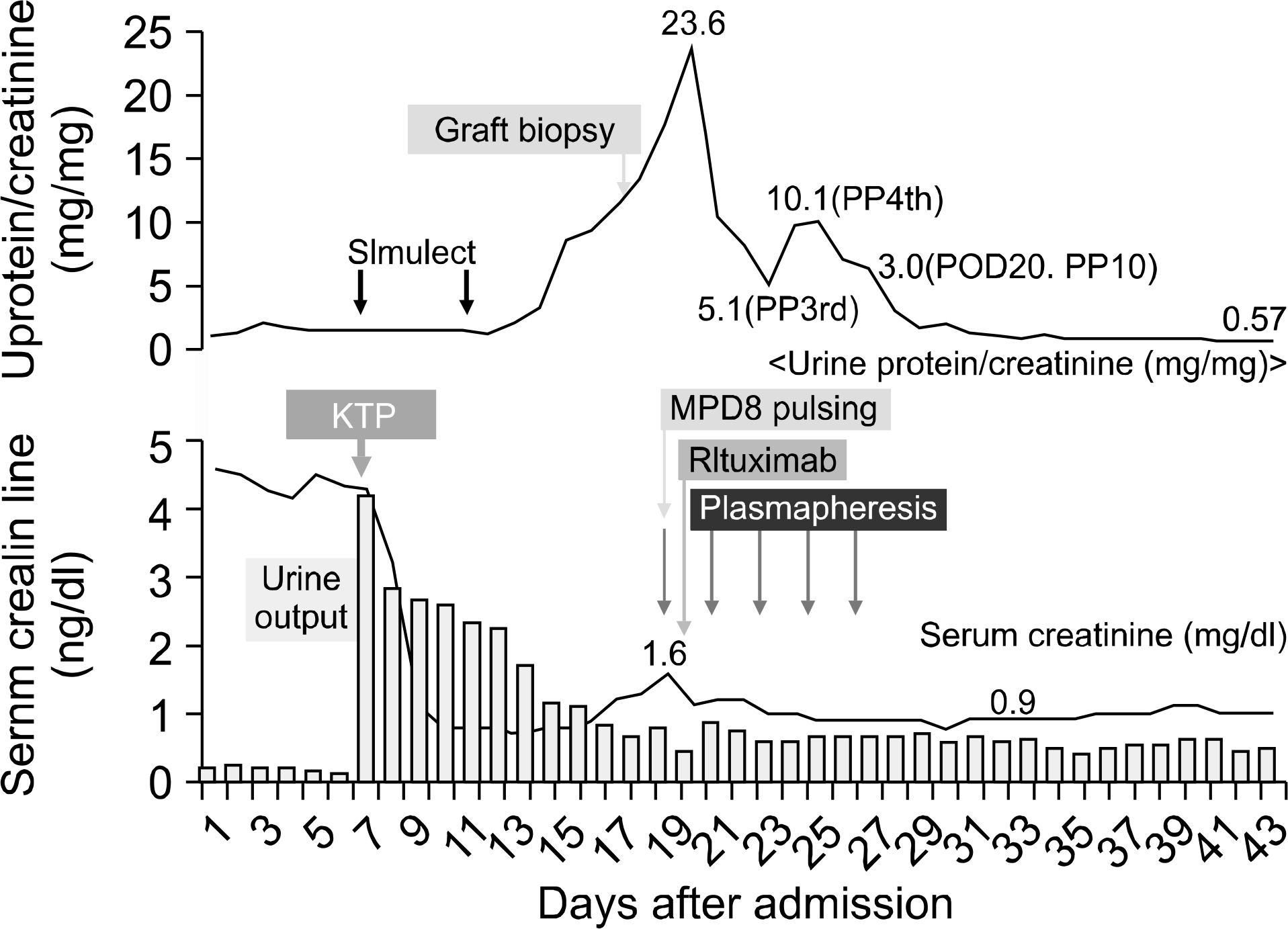
Fig. 6. Clinical course 2. Abbreviations: POD, postoperative days; MPDS, methylprednisolone pulsing.
Reference
-
References
1). Ivanyi B. A primer on recurrent and de novo glomerulonephritis in renal allografts. Nat Clin Pract Nephrol. 2008; 4:446–57.
Article2). Choy BY, Chan TM, Lai KN. Recurrent glomerulonephritis after kidney transplantation. Am J Transplant. 2006; 6:2535–42.
Article3). Savin VJ, Sharma R, Sharma M, McCarthy ET, Swan SK, Ellis E, et al. Circulating factor associated with increased glomerular permeability to albumin in recurrent focal segmental glomerulosclerosis. N Engl J Med. 1996; 334:878–83.
Article4). Artero ML, Sharma R, Savin VJ, Vincenti F. Plasmapheresis reduces proteinuria and serum capacity to injure glomeruli in patients with recurrent focal glomerulosclerosis. Am J Kidney Dis. 1994; 23:574–81.
Article5). Artero M, Biava C, Amend W, Tomlanovich S, Vincenti F. Recurrent focal glomerulosclerosis: natural history and response to therapy. Am J Med. 1992; 92:375–83.
Article6). Friedberg JW. Treatment of follicular non-Hodgkin's lymphoma: the old and the new. Semin Hematol. 2008; 45(3S2):S2–6.
Article7). Zecca M, Nobili B, Ramenghi U, Perrotta S, Amendola G, Rosito P, et al. Rituximab for the treatment of refractory autoimmune hemolytic anemia in children. Blood. 2003; 101:3857–61.
Article8). Blaes AH, Peterson BA, Bartlett N, Dunn DL, Morrison VA. Rituximab therapy is effective for posttransplant lymphoproliferative disorder after solid organ transplantation: results of a phase II trial. Cancer. 2005; 104:1661–7.9). Nozu K, Iijima K, Fujisawa M, Nakagawa A, Yoshikawa N, Matsuo M. Rituximab treatment for posttransplant lymphoproliferative disorder (PTLD) induces complete remission of recurrent nephrotic syndrome. Pediatr Nephrol. 2005; 20:1660–3.
Article10). Pescovitz MD, Book BK, Sidner RA. Resolution of recurrent focal segmental glomerulosclerosis proteinuria after rituximab treatment. N Engl J Med. 2006; 354:1961–3.
Article11). Rydel JJ, Korbet SM, Borok RZ, Schwarz MM. Focal segmental glomerular sclerosis is adults: presentation, course, and response to treatment. Am J Kidney Dis. 1995; 25:534–42.12). Walker RG, Kincaid-Smith P. The effect of treatment of corticosteroid-resistant idiopathic (primary) focal and segmental hyalinosis and sclerosis (focal glomerulosclerosis) with ciclosporin. Nephron. 1990; 54:117–21.
Article13). Sharma M, Sharma R, McCarthy ET, Savin VJ. The focal segmental glomerulosclerosis permeability factor: biochemical characteristics and biological effects. Exp Biol Med (Maywood). 2004; 229:85–98.
Article14). Nakayama M, Kamei K, Nozu K, Matsuoka K, Nakagawa A, Sako M, et al. Rituximab for refractory focal segmental glomerulosclerosis. Pediatr Nephrol. 2008; 23:481–5.
Article15). Kamar N, Faguer S, Esposito L, Guitard J, Nogier MB, Durand D, et al. Treatment of focal segmental glomerular sclerosis with rituximab: 2 case reports. Clin Nephrol. 2007; 67:250–4.
Article16). Srivastava RN, Kalia A, Travis LB, Diven SC, Gugliuzza KK, Rajaraman S. Prompt remission of postrenal transplant nephrotic syndrome with high-dose cyclosporine. Pediatr Nephrol. 1994; 8:94–5.
Article17). Cochat P, Kassir A, Colon S, Glastre C, Tourniaire B, Parchoux B, et al. Recurrent nephrotic syndrome after transplantation: early treatment with plasmaphaeresis and cyclophosphamide. Pediatr Nephrol. 1993; 7:50–4.
Article18). Dantal J, Bigot E, Bogers W, Testa A, Kriaa F, Jacques Y, et al. Effect of plasma protein adsorption on protein excretion in kidney-transplant recipients with recurrent nephrotic syndrome. N Engl J Med. 1994; 330:7–14.
Article19). Weiner GJ, Link BK. Antibody therapy of lymphoma. Adv Pharmacol. 2004; 51:229–53.
Article20). Becker YT, Samaniego-Picota M, Sollinger HW. The emerging role of rituximab in organ transplantation. Transpl Int. 2006; 19:621–8.
Article21). Pescovitz MD. Rituximab, an anti-CD20 monoclonal antibody: history and mechanism of action. Am J Transplant. 2006; 6:859–66.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rituximab and Plasmapheresis for Post-transplant Recurrence of FSGS
- A Case of Successful Third Renal Transplantation Using Rituximab (anti-CD20 Monoclonal Antibody) in a Highly Sensitized Patient
- Prevention of Recurrent FSGS with Cyclosporine and Plasmapheresis Prior to Renal Transplantation
- Plasmapheresis in Recurrent Focal Segmental Glomerulosclerosis after Renal Transplantation
- A Case of Heart Transplant Rejection Treated with Plasmapheresis
