J Korean Soc Endocrinol.
2005 Oct;20(5):502-506. 10.3803/jkes.2005.20.5.502.
A Case Of Transient Hyporeninemic Hypoaldosteronism After Unilateral Adrenalrectomy for Aldosterone-Producing Adenoma
- Affiliations
-
- 1Department of Internal medicine, Kyung Hee university College of Medicine, Seoul, Korea.
- 2Research Institute of Endocrinology, Kyung Hee university College of Medicine, Seoul, Korea.
- 3Department of Endocrinology, College of Medicine, Konyang University, Daejeon, Korea.
- KMID: 2200598
- DOI: http://doi.org/10.3803/jkes.2005.20.5.502
Abstract
- Primary aldosteronism is due to either a unilateral adrenal adenoma or bilateral hyperplasia of the adrenal cortex in most cases. A unilateral adrenalectomy in hypertensive and hypokalemic patients, with a well-documented adrenal adenoma, is usually followed by the correction of hypokalemia in all subjects, with the cure of hypertension in 60 to 87% of patients. Here, a unique case, in which a unilateral adrenalectomy for the removal of an adrenal adenoma was followed by severe hyperkalemia, low levels of plasma renin activity and serum aldosterone, suggestive of chronic suppression of the renin-aldosterone axis, is reported. In a follow-up Lasix stimulation test on the 70th day after surgery, the suppression of the renin-aldosterone axis was resolved, indicating the suppression was transient. Patients undergoing a unilateral adrenalectomy for an aldosterone-producing adenoma should be closely followed up to avoid severe hyperkalemia.
MeSH Terms
Figure
-
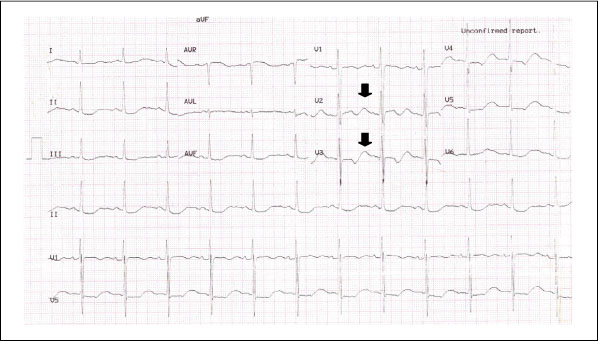
Fig. 1 EKG finding showing hypokalkemic U-wave (The black arrows in V2, V3).
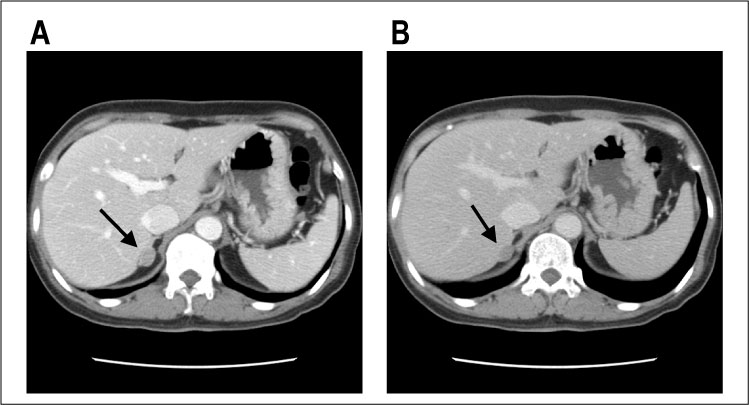
Fig. 2 A. Enhanced (A) and Post-enhanced (B) abdominal CT finding showing a right adrenal mass (the black arrow). B. The two CT films shows a moderately enhanced mass on right adrenal gland. Its size is about 1×1 cm and the nature is homogenous.

Fig. 3-A Gross finding of adrenal adenoma which is circular shaped and golden yellow colored. The wellmarginated circular mass is about 1cm in diameter and contains much lipid. Around the adenoma there is perirenal fat tissue.
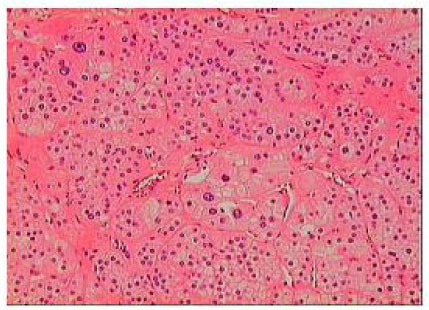
Fig. 3-B Microscopic finding of adrenal adenoma which shows lipid-abundant clear cells and giant cells.
Reference
-
1. Favia G, Lumachi F, Scarpa V, D'Amico DF. Adrenalectomy in primary aldosteronism: a long-term follow-up study in 52 patients. World J Surg. 1992. 16:683–684.2. Irony I, Kater CE, Biglieri EG, Shackleton CH. Correctable subsets of primary aldosteronism: Primary adrenal hyperplasia and renin responsive adenoma. Am J Hypertens. 1990. 3:576–582.3. Grandberg PO, Adamson U, Chon KH, Hamburger H, Lins PE. The management of patients with primary aldosteronism. World J Surg. 1982. 6:757–762.4. Groth H, Vetter H, Stimpel M, Greminger P, Tenschert W, Klaiber E, Vetter H. Adrenalectomy in primary aldosteronism: A long-term follow-up study. Cardiology. 1985. 72:107–112.5. Lim RC Jr, Nakayama DK, Biglieri EG, Schambelan M, Hunt TK. Primary aldosteronism: changing concepts in diagnosis and management. Am J surg. 1986. 152:116–121.6. Bravo EL, Fouad-Tarazi FM, Tarazi RC, Pohl M, Gifford RW, Vidt DG. Clinical implications of primary aldosteronism with resistant hypertension. Hypertension. 1988. 11:207–211.7. Gordon R, Hawkins P, Hamlet S, Tunny T, Klemm S, Bachmann A, Finn W. Reduced adrenal secretory mass after unilateral adrenalectomy for aldosterone-producing adenoma may explain unexpected incidence of hypotension. J Hypertens. 1989. 6:210–211.8. Gadallah MF, Kayyas Y, Boules F. Reversible suppression of the renin-aldosterone axis after unilateral adrenalectomy for adrenal adenoma. Am J Kidney Dis. 1998. 32:160–163.9. Biglieri EG, Slatton PE Jr, Silen WS, Galante M, Forsham PM. Postoperative studies of adrenal function in primary aldosteronism. J Clin Endocrinol. 1966. 26:553–558.10. Morimoto S, Takeda R, Murakami M. Does prolonged pretreatment with large doses of spironolactone hasten a recovery from juxtaglomerular-adrenal suppression in primary aldosteronism. J Clin Endocrinol. 1970. 31:659–664.11. Conn JW, Rovner DR, Cohen EL. Normal and altered function of the renin-angiotensin-aldosterone system in man. Ann Intern Med. 1965. 63:266–284.12. Yodaiken RE, Levin NW, Sandler A. A case of Klinefelter's syndrome complicated by diabetes and glomerulosclerosis. S Afr Med J. 1960. 34:547–550.13. Williams GH, Dluhy RG. Disorders of the adrenal cortx. Harrison's principles of internal medicine. 2004. 16th edition. Philadelphia: McGraw-Hill's;2144–2145.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Persistent Hyperkalemia After Unilateral Adrenalectomy for Aldosterone-Producing Adenoma
- Hyperkalemia due to hyporeninemic hypoaldosteronism with liver cirrhosis and hypertension
- A Case of Diabetic Hyporeninemic Hypoaldosteronism Associated with Muscular Symptoms Due to Hyperkalemia
- A case of idiopathic hyperaldosteronism vs. bilateral aldosterone producing adenoma
- Anesthetic Experience with Primary Aldosteronism: Report of a case
