The Usefulness of CT Brain Perfusion Image on Evaluation of Traumatic Brain Injury
- Affiliations
-
- 1Department of Neurosurgery, Wonju College of Medicine, Yonsei University, Wonju, Korea. whangkum@yonsei.ac.kr
- 2Department of Radiology, Wonju College of Medicine, Yonsei University, Wonju, Korea.
- KMID: 2192353
- DOI: http://doi.org/10.13004/jknts.2010.6.1.6
Abstract
OBJECTIVE
The purpose of this study is to evaluate the finding of computed tomography brain perfusion (CBP) in early traumatic brain injury patient.
METHODS
33 patients with head trauma were evaluated and the patients were classified into 4 categories: traumatic subarachnoid hemorrhage (T-SAH), actue epidural hematoma (EDH), acutue subdural hematoma (SDH), traumatic intracerebral hemorrhage (T-ICH). We evaluated the cerebral blood flow (CBF), cerebral blood volume (CBV), mean transit time (MTT) of the lesion vs contralateral lesion, lesion's hemisphere and brain stem vs contralateral side and compared them.
RESULTS
T-SAH was found in 7 cases. And the all T-SAH patients have no perfusion defect and they have no ischemic change on follow up brain CT. EDH was found in 11 cases. 3 of the 11 EDH patients have perfusion defect that was not revealed by non-contrast CT. According to the EDH size, brain stem perfusion value was different. And at the same size of EDH, the value was low if patients have low initial GCS. SDH was found in 9 cases. The 2 cases have different operation. Decompressive craniectomy was made for one patient who have low perfusion value of brain stem. And osteoplastic craniotomy was made for the other patient who have relative high perfusion value. The low perfusion value of brain stem was correleated with brain swelling. T-ICH was found in 12 cases. Contusion sites have decreased perfusion value and the DTICH (delayed traumatic intracerebral hemorrhage) was developed perfusion defect area on initial CT brain perfusion.
CONCLUSION
The CBP give us meaningful information of traumatic brain injury that associated with patient's unexplained symptom, and may be useful for deciding operative plan, and predicting the prognosis of the patient.
Keyword
MeSH Terms
Figure
-
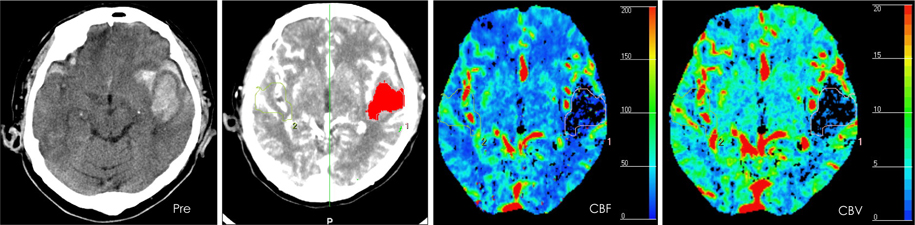
FIGURE 1 The example of ROI setting. The pre contrast CT brain showd the ICH on Lt temporal. The work station showed us source image. We draw the ROI on perfusion defect area of ICH. The CBF, CBV was calculated automatically. ROI: region of interest. ICH: intracerebral hemorrhage, CBF: cerebral blood flow, CBV: cerebral blood volume.

FIGURE 2 Perfusion defect area that not revealed non-contrast CT. The patient contusion site (large arrow) which was not revealed by noncontrast CT.
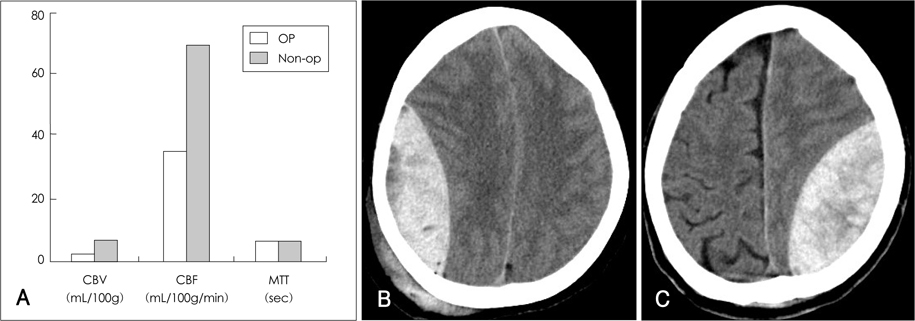
FIGURE 3 The comparison of perfusion value of brain stem in EDH patients. A: The perfusion value of Non-operative group was higher than operative group. B: 38 yrs old female. C: 5 yrs male. B have higher perfusion value of brain stem than C. And Initial GCS of B was also higher than C. CBV: cerebral blood volume, CBF: cerebral blood flow, MTT: mean transit time, EDH: epidural hematoma, GCS: Glasgow Coma Scale.
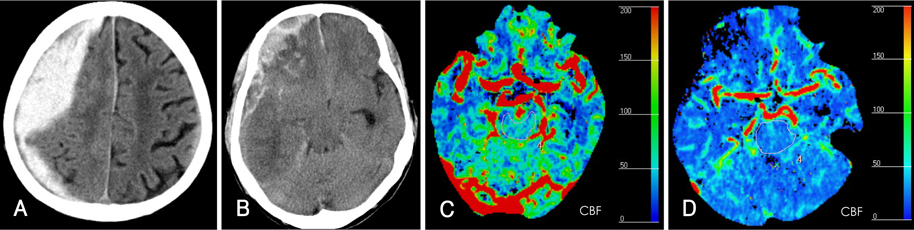
FIGURE 4 The comparison of operation case in acute subdural hematoma. A, C: 95 yrs old male. No brain swelling was noted in operating field. So osteoplastic craniotomy and hematoma evacuation was done. The perfusion value of brain stem was normal range. B, D: 72 yrs old male. Severe brain swelling was noted. And so decompressive craniectomy and hematoma evacuation operation was done. Low perfusion value of brain stem was checked. CBF: cerebral blood flow.
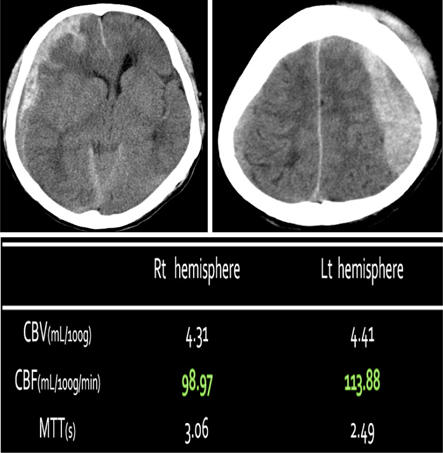
FIGURE 5 The comparison of perfusion value in case that have Right SDH and Left EDH. Both injuries required emergency operation. The sum of perfusion value in right hemisphere was relatively lower than that of Left hemisphere, suggesting that more stress was affecting the right side. SDH: subdural hematoma, EDH: epidural hematoma, CBV: cerebral blood volume, CBF: cerebral blood flow.
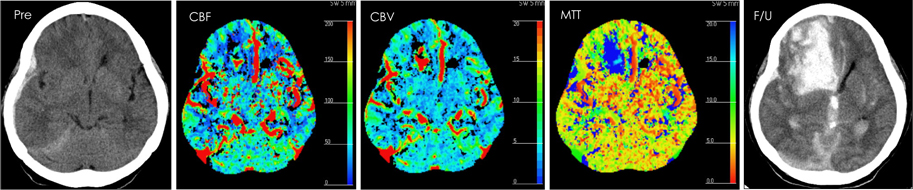
FIGURE 6 DT-ICH on perfusion defect area. On F/U CT brain image, DT-ICH was newly developed on Right Frontal area and that is correlated with initial perfusion defect area. DT-ICH: delayed traumatic intracerebral hemorrhage. F/U: follow up, GCS: Glasgow Coma Scale, CBF: cerebral blood flow, CBV: cerebral blood volume, MTT: mean transit time.
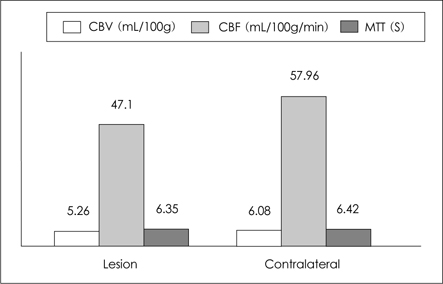
FIGURE 7 Perfusion value of both hemisphere in traumatic brain injury patients. The un injured side's hemisphere had better blood flow and volume than injured side's (Paired t-test, p<0.0142).
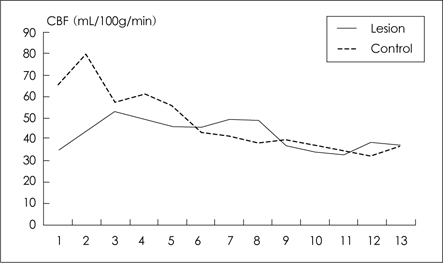
FIGURE 8 Hemorrhage and CBF of all axial cut image in a case. Our calculation showed better CBF in the control group as a whole. However, in one or two axial images, flows on lesion resulted better than the control group. CBF: cerebral blood flow.
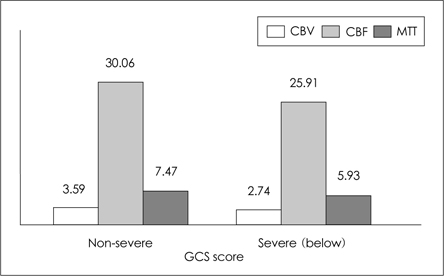
FIGURE 9 Mental status and brain stem perfusion. The CBF and CBV of non-severe group were higher than severe group. But no statistical importance was found. CBV: cerebral blood volume, CBF: cerebral blood flow, MTT: mean transit time, GCS: Glasgow Coma Scale.
Reference
-
1. Andrews BT, Chiles BW 3rd, Olsen WL, Pitts LH. The effect of intracerebral hematoma location on the risk of brain-stem compression and on clinical outcome. J Neurosurg. 1988; 69:518–522.
Article2. Barzó P, Marmarou A, Fatouros P, Hayasaki K, Corwin F. Contribution of vasogenic and cellular edema to traumatic brain swelling measured by diffusion-weighted imaging. J Neurosurg. 1997; 87:900–907.
Article3. Fukamachi A, Nagaseki Y, Kohno K, Wakao T. The incidence and developmental process of delayed traumatic intracerebral haematomas. Acta Neurochir (Wien). 1985; 74:35–39.
Article4. Gudeman SK, Kishore PR, Miller JD, Girevendulis AK, Lipper MH, Becker DP. The genesis and significance of delayed traumatic intracerebral hematoma. Neurosurgery. 1979; 5:309–313.
Article5. Komeda Y, Kato H, Saito K, Morishita F, Mori Y. [Adverse effect of iodine contrast media.]. Hinyokika Kiyo. 1987; 33:183–186.6. Koide M, Nishizawa S, Ohta S, Yokoyama T, Namba H. Chronological changes of the contractile mechanism in prolonged vasospasm after subarachnoid hemorrhage: from protein kinase C to protein tyrosine kinase. Neurosurgery. 2002; 51:1468–1474. discussion 1474-1476.
Article7. Kim JT, Shin DS, Nam TS, Jung ES, Choi SM, Son EJ, et al. Clinical usefulness of perfusion CT in acute ischemic stroke. J Korean Neurol Assoc. 2002; 20:585–591.8. Kim PG, Whang K, Cho SM, Kim HJ, Lee MS, Kim MS. Perfusion brain magnetic resonance image in patients of head trauma. J Korean Neurosurg Soc. 2002; 32:448–452.9. Martin NA, Patwardhan RV, Alexander MJ, Africk CZ, Lee JH, Shalmon E, et al. Characterization of cerebral hemodynamic phases following severe head trauma: hypoperfusion, hyperemia, and vasospasm. J Neurosurg. 1997; 87:9–19.
Article10. Sander D, Klingelhöfer J. Cerebral vasospasm following post-traumatic subarachnoid hemorrhage evaluated by transcranial Doppler ultrasonography. J Neurol Sci. 1993; 119:1–7.
Article11. Smith DH, Meaney DF, Lenkinski RE, Alsop DC, Grossman R, Kimura H, et al. New magnetic resonance imaging techniques for the evaluation of traumatic brain injury. J Neurotrauma. 1995; 12:573–577.
Article12. Wintermark M, van Melle G, Schnyder P, Revelly JP, Porchet F, Regli L, Meuli R, Maeder P, Chiolero R. Admission perfusion CT: prognostic value in patients with severe head trauma. Radiology. 2004; 232:211–220.
Article13. Wu CW, Liu HL, Chen JH, Yang Y. Effects of CBV, CBF, and blood-brain barrier permeability on accuracy of PASL and VASO measurement. Magn Reson Med. 2010; 63:601–608.
Article14. Xie A, Aihara Y, Bouryi VA, Nikitina E, Jahromi BS, Zhang ZD, et al. Novel mechanism of endothelin-1-induced vasospasm after subarachnoid hemorrhage. J Cereb Blood Flow Metab. 2007; 27:1692–1701.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Initial Evaluation of Patients with Head Injury using CT Brain Perfusion Imaging in the Emergency Room: Two Cases
- The Role of Tc-99m HMPAO Brain Perfusion SPECT in the Psychiatric Disability Evaluation of Patients with Chronic Traumatic Brain Injury
- Traumatic Brain injury and Sleep Disorder
- Animal Models of Traumatic Brain Injury
- Anesthetic management of the traumatic brain injury patients undergoing non-neurosurgery
