Comparison of Clinical and Radiologic Results between Expandable Cages and Titanium Mesh Cages for Thoracolumbar Burst Fracture
- Affiliations
-
- 1Department of Neurosurgery, Chonnam National University Research Institute of Medical Sciences, Chonnam National University Hospital & Medical School, Gwangju, Korea. jkl@chonnam.ac.kr
- KMID: 2191079
- DOI: http://doi.org/10.3340/jkns.2014.55.3.142
Abstract
OBJECTIVE
A thoracolumbar burst fracture is usually unstable and can cause neurological deficits and angular deformity. Patients with unstable thoracolumbar burst fracture usually need surgery for decompression of the spinal canal, correction of the angular deformity, and stabilization of the spinal column. We compared two struts, titanium mesh cages (TMCs) and expandable cages.
METHODS
33 patients, who underwent anterior thoracolumbar reconstruction using either TMCs (n=16) or expandable cages (n=17) between June 2000 and September 2011 were included in this study. Clinical outcome was measured by visual analogue scale (VAS), American Spinal Injury Association (ASIA) scale and Low Back Outcome Score (LBOS) for functional neurological evaluation. The Cobb angle, body height of the fractured vertebra, the operation time and amount of intra-operative bleeding were measured in both groups.
RESULTS
In the expandable cage group, operation time and amount of intraoperative blood loss were lower than that in the TMC group. The mean VAS scores and LBOS in both groups were improved, but no significant difference. Cobb angle was corrected higher than that in expandable cage group from postoperative to the last follow-up. The change in Cobb angles between preoperative, postoperative, and the last follow-up did not show any significant difference. There was no difference in the subsidence of anterior body height between both groups.
CONCLUSION
There was no significant difference in the change in Cobb angles with an inter-group comparison, the expandable cage group showed better results in loss of kyphosis correction, operation time, and amount of intraoperative blood loss.
Keyword
MeSH Terms
Figure
-
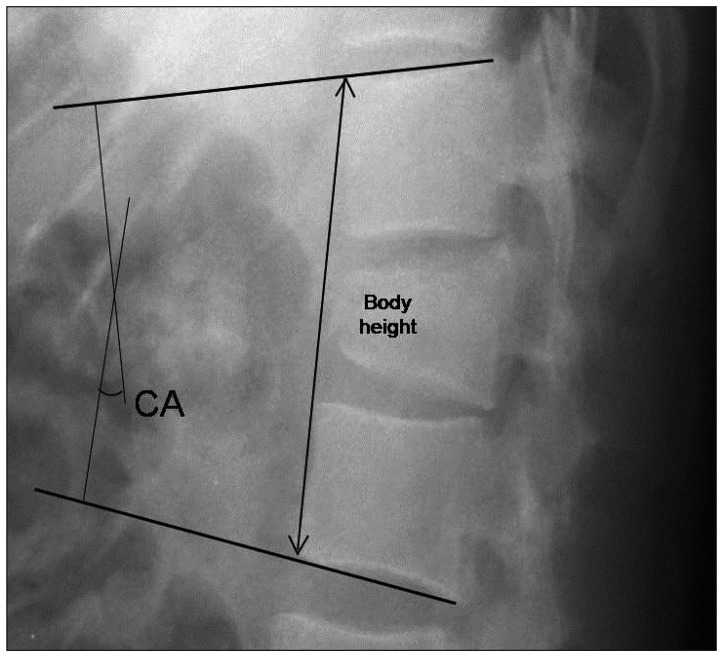
Fig. 1 Radiologic findings. Sagittal Cobb angle (CA) and vertebral body height.
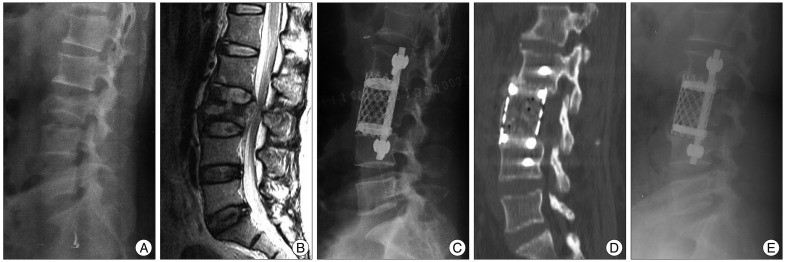
Fig. 2 Case presentation 1. A : A 42-year-old woman sustained an L3 burst fracture after a fall. Lateral plain radiograph before the operation. B : Sagittal magnetic resonance imaging of the lumbar spine shows loss of height of the 3rd lumbar vertebra and bony retropulsion into the spinal canal. The Cobb angle was 7.71 degrees and anterior vertebral body height was 126.1 mm. C : With the use of a TMC, immediate post-operative lateral plain radiograph shows good implant placement with a Cobb angle of 10.21 degrees. D : One-year follow-up computed tomographic image shows solid fusion. E : On a lateral plain radiograph, -5.5 degrees of loss of kyphosis correction is observed.
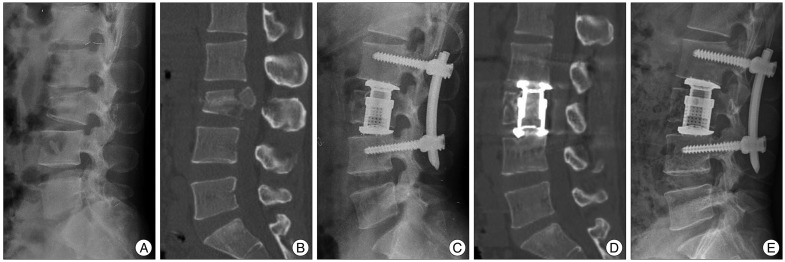
Fig. 3 Case presentation 2. A : A 30-year-old man sustained an L3 burst fracture after a traffic accident. Lateral plain radiograph before the operation. B : Sagittal computed tomographic image of the lumbar spine showing vertebral height loss and bony retropulsion into the spinal canal. The Cobb angle was -6.19 degrees and anterior vertebral body height was 114.3 mm. C : With the use of an expandable cage, immediate post-operative lateral plain radiograph shows good implant placement with a Cobb angle of 12.71 degrees. D : One year follow-up computed tomographic image shows solid fusion. E : One year follow-up computed tomographic image shows solid fusion.
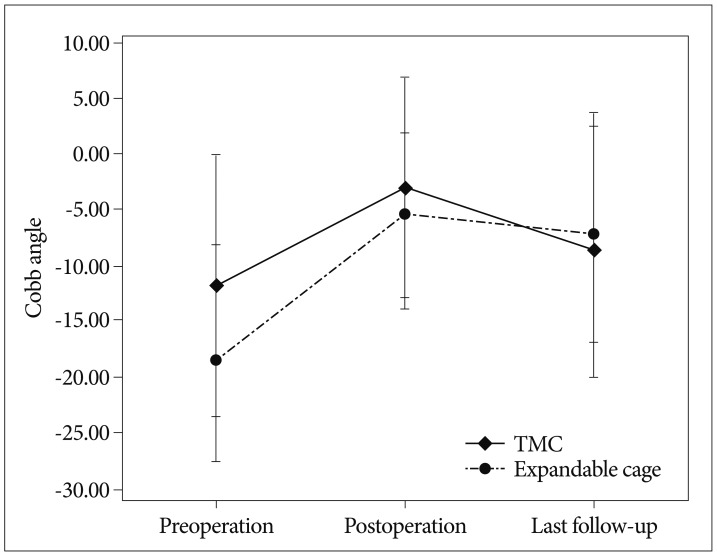
Fig. 4 The change in the Cobb angle between the TMC and expandable cage groups in the preoperative, postoperative and last follow-up periods. TMC : titanium mesh cage.
Cited by 1 articles
-
Single-Stage Posterior Subtotal Corpectomy and Circumferential Reconstruction for the Treatment of Unstable Thoracolumbar Burst Fractures
Dae-Jean Jo, Ki-Tack Kim, Sung-Min Kim, Sang-Hun Lee, Myung-Guk Cho, Eun-Min Seo
J Korean Neurosurg Soc. 2016;59(2):122-128. doi: 10.3340/jkns.2016.59.2.122.
Reference
-
1. Alanay A, Acaroglu E, Yazici M, Oznur A, Surat A. Short-segment pedicle instrumentation of thoracolumbar burst fractures : does transpedicular intracorporeal grafting prevent early failure? Spine (Phila Pa 1976). 2001; 26:213–217. PMID: 11154543.2. Boriani S, Biagini R, Bandiera S, Gasbarrini A, De Iure F. Reconstruction of the anterior column of the thoracic and lumbar spine with a carbon fiber stackable cage system. Orthopedics. 2002; 25:37–42. PMID: 11811240.
Article3. Ditunno JF Jr, Young W, Donovan WH, Creasey G. The international standards booklet for neurological and functional classification of spinal cord injury. American Spinal Injury Association. Paraplegia. 1994; 32:70–80. PMID: 8015848.
Article4. Dvorak MF, Kwon BK, Fisher CG, Eiserloh HL 3rd, Boyd M, Wing PC. Effectiveness of titanium mesh cylindrical cages in anterior column reconstruction after thoracic and lumbar vertebral body resection. Spine (Phila Pa 1976). 2003; 28:902–908. PMID: 12942006.
Article5. Eck KR, Bridwell KH, Ungacta FF, Lapp MA, Lenke LG, Riew KD. Analysis of titanium mesh cages in adults with minimum two-year follow-up. Spine (Phila Pa 1976). 2000; 25:2407–2415. PMID: 10984797.
Article6. Eleraky MA, Duong HT, Esp E, Kim KD. Expandable versus nonexpandable cages for thoracolumbar burst fracture. World Neurosurg. 2011; 75:149–154. PMID: 21492680.
Article7. Finkelstein JA, Chapman JR, Mirza S. Anterior cortical allograft in thoracolumbar fractures. J Spinal Disord. 1999; 12:424–429. PMID: 10549708.
Article8. Hitchon PW, Torner J, Eichholz KM, Beeler SN. Comparison of anterolateral and posterior approaches in the management of thoracolumbar burst fractures. J Neurosurg Spine. 2006; 5:117–125. PMID: 16925077.
Article9. Kaneda K, Taneichi H, Abumi K, Hashimoto T, Satoh S, Fujiya M. Anterior decompression and stabilization with the Kaneda device for thoracolumbar burst fractures associated with neurological deficits. J Bone Joint Surg Am. 1997; 79:69–83. PMID: 9010188.
Article10. Kim MS, Eun JP, Park JS. Radiological and clinical results of laminectomy and posterior stabilization for severe thoracolumbar burst fracture : surgical technique for one-stage operation. J Korean Neurosurg Soc. 2011; 50:224–230. PMID: 22102953.
Article11. Knop C, Lange U, Bastian L, Blauth M. Three-dimensional motion analysis with Synex. Comparative biomechanical test series with a new vertebral body replacement for the thoracolumbar spine. Eur Spine J. 2000; 9:472–485. PMID: 11189915.12. Krompinger WJ, Fredrickson BE, Mino DE, Yuan HA. Conservative treatment of fractures of the thoracic and lumbar spine. Orthop Clin North Am. 1986; 17:161–170. PMID: 3945477.
Article13. Lau D, Song Y, Guan Z, La Marca F, Park P. Radiological outcomes of static vs expandable titanium cages after corpectomy : a retrospective cohort analysis of subsidence. Neurosurgery. 2013; 72:529–539. discussion 528-529. PMID: 23246824.
Article14. Miyakoshi N, Abe E, Shimada Y, Hongo M, Chiba M, Sato K. Anterior decompression with single segmental spinal interbody fusion for lumbar burst fracture. Spine (Phila Pa 1976). 1999; 24:67–73. PMID: 9921594.
Article15. Mumford J, Weinstein JN, Spratt KF, Goel VK. Thoracolumbar burst fractures. The clinical efficacy and outcome of nonoperative management. Spine (Phila Pa 1976). 1993; 18:955–970. PMID: 8367783.16. Payer M. Unstable burst fractures of the thoraco-lumbar junction : treatment by posterior bisegmental correction/fixation and staged anterior corpectomy and titanium cage implantation. Acta Neurochir (Wien). 2006; 148:299–306. discussion 306. PMID: 16311837.
Article17. Uchida K, Kobayashi S, Nakajima H, Kokubo Y, Yayama T, Sato R, et al. Anterior expandable strut cage replacement for osteoporotic thoracolumbar vertebral collapse. J Neurosurg Spine. 2006; 4:454–462. PMID: 16776356.
Article18. Wang ST, Ma HL, Liu CL, Yu WK, Chang MC, Chen TH. Is fusion necessary for surgically treated burst fractures of the thoracolumbar and lumbar spine? : a prospective, randomized study. Spine (Phila Pa 1976). 2006; 31:2646–2652. discussion 2653. PMID: 17077731.
Article19. Wood KB, Bohn D, Mehbod A. Anterior versus posterior treatment of stable thoracolumbar burst fractures without neurologic deficit : a prospective, randomized study. J Spinal Disord Tech. 2005; 18(Suppl):s15–s23. PMID: 15699801.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Radiological and Clinical Outcomes between Expandable and Non-expandable Cages Following Cervical Corpectomy: A Systematic Review and Meta-analysis
- One Stage Decompression and Circumferential Stabilization by Posterior Approach in the Unstable Burst Fracture of Thoracolumbar and Lumbar Spine
- Efficacy of Titanium Mesh Cage for Anterior Spinal Reconstruction after Thoracolumbar Corpectomy
- Comparison of Titanium Micro Mesh(R) with Titanium Mesh Screen 1.3(R) in the Reconstruction of Medial Orbital wall Fracture
- Future Development of Interbody Fusion Cages
