J Korean Med Assoc.
2011 Feb;54(2):181-186. 10.5124/jkma.2011.54.2.181.
The surgical treatment for type 2 diabetes mellitus
- Affiliations
-
- 1Department of Surgery, Soonchunhyang University College of Medicine, Seoul, Korea. hurusa@hanmail.net
- KMID: 2189141
- DOI: http://doi.org/10.5124/jkma.2011.54.2.181
Abstract
- Type 2 diabetes mellitus (T2DM) has become an epidemic. Compared to Western countries, Asian T2DM occurs in patients with a lower body mass index, due to central obesity and decreased pancreatic beta-cell function. The efficacy of surgical treatment such as sleeve gastrectomy, adjustable gastric banding, and gastric bypass in obese patients with T2DM has been demonstrated by numerous studies from Western countries. However, current evidence on surgical treatment for non-morbidly obese diabetic patients is lacking. Recently, several preliminary studies demonstrated the remission of hyperglycemia in non-obese T2DM patients by surgical bypass. One possible hypothesis is the foregut theory an inactivation of the anti-incretin system through the exclusion of the foregut from ingested food, and the other is the hindgut theory, in which rapid hindgut exposure prompts the delivery of undigested food to the terminal ileum and promotes the activation of incretin system such as glucagon-like peptide-1 The following teaching points and direction of future study are recommended: understanding the mechanism of diabetic remission through surgical procedure, defining the surgical indications for T2DM, predicting the possible complications and disadvantages of surgical treatment, and understanding the peculiarity of each surgical procedure. The remission of hyperglycemia in non-obese T2DM patients could possibly be achieved by surgical intervention. Although long-term follow-up data and verification of its exact mechanisms are required, early operative outcomes were satisfactory in terms of glycemic control and the safety of the procedure.
Keyword
MeSH Terms
Figure
-
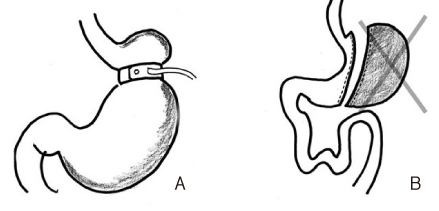
Figure 1 Restrictive surgery. (A) Adjustable gastric banding. (B) Gastric sleeve resection.

Figure 2 Restrictive and malaborptive surgery and malabsoptive surgery. (A) Roux-en-Y gastric bypass. (B) Mini-gastric bypass. (C) Duodeno-jejunal bypass.
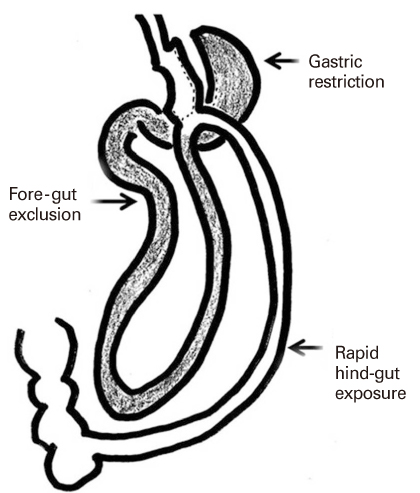
Figure 3 The surgical mechanism of type 2 diabetes treatment.

Figure 4 HbA1c for 6 months showed a continuous decrease after mini-gastric bypass (From Kim Z, Hur KY. World J Surg 2010 Dec 17 [Epub], with permission from Springer) [23].
Reference
-
1. Yang W, Lu J, Weng J, Jia W, Ji L, Xiao J, Shan Z, Liu J, Tian H, Ji Q, Zhu D, Ge J, Lin L, Chen L, Guo X, Zhao Z, Li Q, Zhou Z, Shan G, He J. China National Diabetes and Metabolic Disor-ders Study Group. Prevalence of diabetes among men and women in China. N Engl J Med. 2010. 362:1090–1101.
Article2. Yoon KH, Lee JH, Kim JW, Cho JH, Choi YH, Ko SH, Zimmet P, Son HY. Epidemic obesity and type 2 diabetes in Asia. Lancet. 2006. 368:1681–1688.
Article3. Pories WJ, Swanson MS, MacDonald KG, Long SB, Morris PG, Brown BM, Barakat HA, deRamon RA, Israel G, Dolezal JM, Dohm L. Who would have thought it? An operation pro-ves to be the most effective therapy for adult-onset diabetes mellitus. Ann Surg. 1995. 222:339–350.
Article4. Pories WJ, MacDonald KG Jr, Flickinger EG, Dohm GL, Sinha MK, Barakat HA, May HJ, Khazanie P, Swanson MS, Morgan E, Leggett-Frazier N, Long SD, Brown BM, O'Brien K, Caro JF. Is type II diabetes mellitus (NIDDM) a surgical disease? Ann Surg. 1992. 215:633–642.
Article5. Madan AK, Orth W, Ternovits CA, Tichansky DS. Metabolic syndrome: yet another co-morbidity gastric bypass helps cure. Surg Obes Relat Dis. 2006. 2:48–51.
Article6. Rubino F, Forgione A, Cummings DE, Vix M, Gnuli D, Mingrone G, Castagneto M, Marescaux J. The mechanism of diabetes control after gastrointestinal bypass surgery reveals a role of the proximal small intestine in the pathophysiology of type 2 diabetes. Ann Surg. 2006. 244:741–749.
Article7. Hickey MS, Pories WJ, MacDonald KG Jr, Cory KA, Dohm GL, Swanson MS, Israel RG, Barakat HA, Considine RV, Caro JF, Houmard JA. A new paradigm for type 2 diabetes mellitus: could it be a disease of the foregut? Ann Surg. 1998. 227:637–643.8. Lee H, Kim M, Kwon H, Song K, Kim E. The impact of metabolic and bariatric surgery on morbidly obese patients with type 2 DM. J Korean Surg Soc. 2010. 79:8–13.
Article9. Singhal R, Bryant C, Kitchen M, Khan KS, Deeks J, Guo B, Super P. Band slippage and erosion after laparoscopic gastric banding: a meta-analysis. Surg Endosc. 2010. 24:2980–2986.
Article10. Regan JP, Inabnet WB, Gagner M, Pomp A. Early experience with two-stage laparoscopic Roux-en-Y gastric bypass as an alternative in the super-super obese patient. Obes Surg. 2003. 13:861–864.
Article11. Almogy G, Crookes PF, Anthone GJ. Longitudinal gastrectomy as a treatment for the high-risk super-obese patient. Obes Surg. 2004. 14:492–497.
Article12. Tagaya N, Kasama K, Kikkawa R, Kanahira E, Umezawa A, Oshiro T, Negishi Y, Kurokawa Y, Nakazato T, Kubota K. Experience with laparoscopic sleeve gastrectomy for morbid versus super morbid obesity. Obes Surg. 2009. 19:1371–1376.
Article13. No JH, Kim Z, Kim YJ, Cho SW, Choi DH, Hur KY, Kim JJ. Initial experience of laparoscopic sleeve gastrectomy in morbidly obese patients. J Korean Surg Soc. 2010. 79:460–466.
Article14. Baltasar A, Serra C, Perez N, Bou R, Bengochea M. Re-sleeve gastrectomy. Obes Surg. 2006. 16:1535–1538.
Article15. Sabiston DC, Townsend CM. Sabiston textbook of surgery: the biological basis of surgical practice. 2008. 18th ed. Philadelphia: Sanunders Elsevier.16. Marshall JS, Srivastava A, Gupta SK, Rossi TR, DeBord JR. Roux-en-Y gastric bypass leak complications. Arch Surg. 2003. 138:520–523.
Article17. Nguyen NT, Huerta S, Gelfand D, Stevens CM, Jim J. Bowel obstruction after laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2004. 14:190–196.
Article18. Lee WJ, Yu PJ, Wang W, Chen TC, Wei PL, Huang MT. Laparoscopic Roux-en-Y versus mini-gastric bypass for the treatment of morbid obesity: a prospective randomized controlled clinical trial. Ann Surg. 2005. 242:20–28.
Article19. Johnson WH, Fernanadez AZ, Farrell TM, Macdonald KG, Grant JP, McMahon RL, Pryor AD, Wolfe LG, DeMaria EJ. Surgical revision of loop ("mini") gastric bypass procedure: multicenter review of complications and conversions to Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2007. 3:37–41.
Article20. Rubino F, Marescaux J. Effect of duodenal-jejunal exclusion in a non-obese animal model of type 2 diabetes: a new perspec-tive for an old disease. Ann Surg. 2004. 239:1–11.
Article21. Bose M, Olivan B, Teixeira J, Pi-Sunyer FX, Laferrere B. Do Incretins play a role in the remission of type 2 diabetes after gastric bypass surgery: what are the evidence? Obes Surg. 2009. 19:217–229.
Article22. Lee WJ, Wang W, Lee YC, Huang MT, Ser KH, Chen JC. Effect of laparoscopic mini-gastric bypass for type 2 diabetes mellitus: comparison of BMI>35 and <35 kg/m2. J Gastrointest Surg. 2008. 12:945–952.
Article23. Kim Z, Hur KY. Laparoscopic mini-gastric bypass for type 2 diabetes: the preliminary report. World J Surg. 2010. 12. 17. [Epub]. DOI: 10.1007/s00268-010-0909-2.
Article24. Mui W, Lee WJ. Programme book, 6th International Congress of the Asia-Pacific Metabolic and Bariatric Surgical Society [Internet]. Asian consensus for diabetic surgery: report from 1st Asian Diabetic Surgery Summit (ADSS). 2010. cited 2010 Dec 14. Singapore: Asia-Pacific Metabolic and Bariatric Surgical Society;Available from: http://www.apmbss2010.com.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Progressive Decline of beta-cell Function in Type 2 Diabetes Mellitus
- Genetics in Diabetes Mellitus - Contribution to the Classification and Management
- Genetic Diseases Associated with Diabetes Mellitus
- A Case of Newly Diagnosed Type 2 Diabetes Mellitus with Daily Headaches
- Smoking and Type 2 Diabetes Mellitus
