J Korean Orthop Assoc.
2012 Oct;47(5):353-359. 10.4055/jkoa.2012.47.5.353.
A Comparison of Overgrowth after Treatment for Pediatric Femoral Shaft Fractures: Flexible Intramedullary Nailing versus External Fixation
- Affiliations
-
- 1Department of Orthopedic Surgery, Eulji University College of Medicine, Daejeon, Korea. smlee@eulji.ac.kr
- KMID: 2185319
- DOI: http://doi.org/10.4055/jkoa.2012.47.5.353
Abstract
- PURPOSE
Overgrowth is a common complication after the treatment of pediatric femoral fractures. However, the effect of treatment methods on the overgrowth is controversial. We compared the amount of overgrowth between flexible intramedullary nailing and external fixation.
MATERIALS AND METHODS
Twenty-six children with femoral diaphyseal fractures after a minimum 2 year follow-up were enrolled in this retrospective study. Thirteen patients were treated with flexible intramedullary nailing (FIN) group, and the other 13 patients were treated with external fixation (EF) group. The overgrowth of femur, clinical outcomes, and complications were evaluated.
RESULTS
Union was obtained in all patients without major complications, except for overgrowth. Average overgrowth at the 2-year follow-up was 4 mm (-6-13 mm) in the FIN group, and 3 mm (-13-13 mm) in the EF group (p=0.532). Overgrowths of more than 10 mm were observed in four patients; three patients in the FIN group, and one in the EF group.
CONCLUSION
FIN and EF showed similar amounts of overgrowth, after the treatment for pediatric femoral fractures.
MeSH Terms
Figure
-
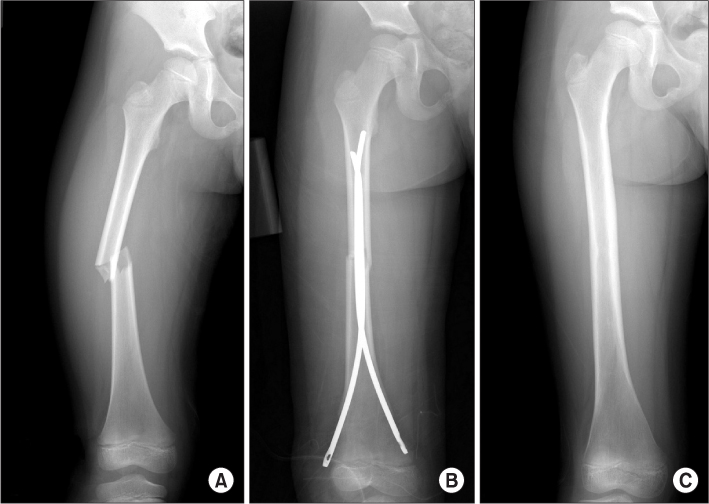
Figure 1 (A) A transverse diaphyseal femoral fracture in a 7-year-old boy. (B) Flexible intramedullary nail was applied. (C) Radiograph at 14 months after the fracture.

Figure 2 (A) A transverse diaphyseal femoral fracture in a 7-year-old boy. (B) External fixator was applied. (C) Radiograph at 15 months after the fracture.
Reference
-
1. Hughes BF, Sponseller PD, Thompson JD. Pediatric femur fractures: effects of spica cast treatment on family and community. J Pediatr Orthop. 1995. 15:457–460.
Article2. Greisberg J, Bliss MJ, Eberson CP, Solga P, d'Amato C. Social and economic benefits of flexible intramedullary nails in the treatment of pediatric femoral shaft fractures. Orthopedics. 2002. 25:1067–1070.
Article3. Evanoff M, Strong ML, MacIntosh R. External fixation maintained until fracture consolidation in the skeletally immature. J Pediatr Orthop. 1993. 13:98–101.
Article4. Flynn JM, Luedtke LM, Ganley TJ, et al. Comparison of titanium elastic nails with traction and a spica cast to treat femoral fractures in children. J Bone Joint Surg Am. 2004. 86:770–777.
Article5. Park SS, Park JB. Comparison of flexible intramedullary nailing with external fixation for treating pediatric femoral shaft fractures. J Korean Orthop Assoc. 2008. 43:665–671.
Article6. Bar-On E, Sagiv S, Porat S. External fixation or flexible intramedullary nailing for femoral shaft fractures in children. A prospective, randomised study. J Bone Joint Surg Br. 1997. 79:975–978.7. Reynolds DA. Growth changes in fractured long-bones: a study of 126 children. J Bone Joint Surg Br. 1981. 63:83–88.
Article8. Stilli S, Magnani M, Lampasi M, Antonioli D, Bettuzzi C, Donzelli O. Remodelling and overgrowth after conservative treatment for femoral and tibial shaft fractures in children. Chir Organi Mov. 2008. 91:13–19.
Article9. Jawish R, Kahwaji A, Dagher G. Overgrowth of femoral fractures in childhood. Rev Chir Orthop Reparatrice Appar Mot. 2003. 89:404–406.10. Galpin RD, Willis RB, Sabano N. Intramedullary nailing of pediatric femoral fractures. J Pediatr Orthop. 1994. 14:184–189.
Article11. Flynn JM, Hresko T, Reynolds RA, Blasier RD, Davidson R, Kasser J. Titanium elastic nails for pediatric femur fractures: a multicenter study of early results with analysis of complications. J Pediatr Orthop. 2001. 21:4–8.
Article12. Ligier JN, Metaizeau JP, Prévot J, Lascombes P. Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br. 1988. 70:74–77.
Article13. Linhart WE, Roposch A. Elastic stable intramedullary nailing for unstable femoral fractures in children: preliminary results of a new method. J Trauma. 1999. 47:372–378.14. Kapukaya A, Subaşi M, Necmioğlu S, Arslan H, Kesemenli C, Yildirim K. Treatment of closed femoral diaphyseal fractures with external fixators in children. Arch Orthop Trauma Surg. 1998. 117:387–389.
Article15. Miner T, Carroll KL. Outcomes of external fixation of pediatric femoral shaft fractures. J Pediatr Orthop. 2000. 20:405–410.
Article16. Gregory P, Pevny T, Teague D. Early complications with external fixation of pediatric femoral shaft fractures. J Orthop Trauma. 1996. 10:191–198.
Article17. Stephens MM, Hsu LC, Leong JC. Leg length discrepancy after femoral shaft fractures in children. Review after skeletal maturity. J Bone Joint Surg Br. 1989. 71:615–618.
Article18. Shannak AO. Tibial fractures in children: follow-up study. J Pediatr Orthop. 1988. 8:306–310.19. Gascó J, de Pablos J. Bone remodeling in malunited fractures in children. Is it reliable? J Pediatr Orthop B. 1997. 6:126–132.
Article20. Shapiro F. Fractures of the femoral shaft in children. The overgrowth phenomenon. Acta Orthop Scand. 1981. 52:649–655.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Flexible Intramedullary Nailing with External Fixation for Treating Pediatric Femoral Shaft Fractures
- Comparison of Flexible Intramedullary Nailing with External Fixation in Pediatric Femoral Shaft Fractures
- Treatment of Open Type-III Tibial Shaft Fractures -Comparison Between Ilizarov External Fixation and Secondary Intramedullary Nailing-
- Operative Treatment in Fractures of the Humeral Shaft: Comparison of the Clinical Results of Flexible Intramedullary Nailing Versus Interlocking Intramedullary Nailing
- Reamed versus Unreamed Intramedullary Nailing after External Fixator Application in the Treatment of Open Tibial-Shaft Fracture
