J Korean Orthop Assoc.
2008 Dec;43(6):665-671.
Comparison of Flexible Intramedullary Nailing with External Fixation for Treating Pediatric Femoral Shaft Fractures
- Affiliations
-
- 1Department of Orthopedic Surgery, Asan Medical Center, Ulsan University Medical College, Seoul, Korea. sspark@amc.seoul.kr
Abstract
-
PURPOSE: We wanted to compare the outcome of the flexible intramedullary nailing with that of external fixation for treating pediatric femoral shaft fractures.
MATERIALS AND METHODS
Forty-two cases of pediatric femoral shaft fractures were reviewed of which thirty cases of femoral segments were treated with the flexible intramedullary nailing (the FIN group) and the other 12 cases were treated with the external fixation (the EF group). The average age of the patients was 6.9 years and the mean follow-up was 28.8 months. The clinical outcome and complications were evaluated.
RESULTS
In all cases, the reduction was maintained until complete union. In the FIN group there were 20 excellent, 8 satisfactory and 2 poor results whereas there were 6 excellent, 4 satisfactory and 2 poor results in the EF group. Among the complications that required re-admission, there was one case of refracture and one case of deep infection in FIN group; one case of refracture, one case of pin breakage and three cases of deep infections in the EF group.
CONCLUSION
Flexible intramedullary nailing may result in better clinical results and fewer complications when compared with the external fixation, and so the flexible intramedullary nailing may be the treatment of choice for the treatment of pediatric femoral shaft fractures, except for open fractures or fractures with severe soft tissue injury.
Figure
-

Fig. 1 A transverse diaphyseal femoral fracture in a 5-year-old boy (A). Flexible intramedullary nailing was applied (B). After five months, the implant was removed (C).
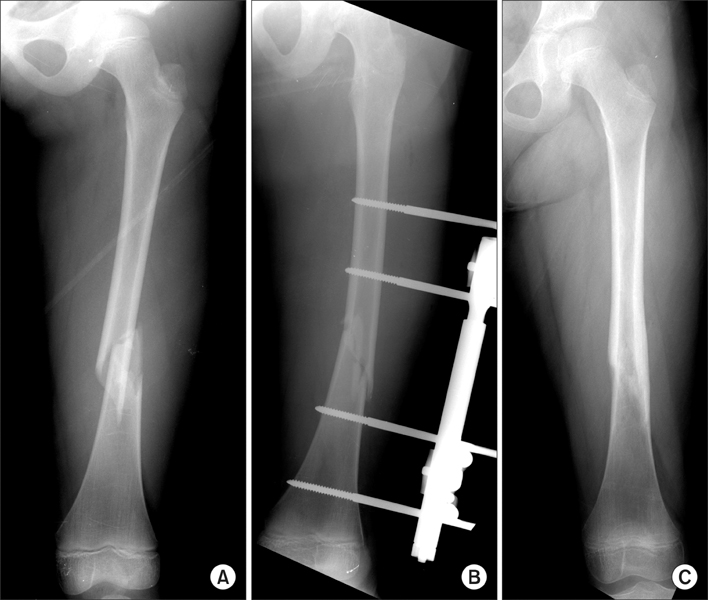
Fig. 2 Fracture of the left femoral diaphysis in an 9-year-old boy (A), and this was treated with external fixation (B). The picture on the right shows the femur after fracture healing and removal of the implant (C).
Reference
-
1. Aronson J, Tursky EA. External fixation of femur fractures in children. J Pediatr Orthop. 1992. 12:157–163.
Article2. Bar-On E, Sagiv S, Porat S. External fixation or flexible intramedullary nailing for femoral shaft fractures in children. A prospective, randomised study. J Bone Joint Surg Br. 1997. 79:975–978.3. Bopst L, Reinberg O, Lutz N. Femur fracture in preschool children: experience with flexible intramedullary nailing in 72 children. J Pediatr Orthop. 2007. 27:299–303.4. Buechsenschuetz KE, Mehlman CT, Shaw KJ, Crawford AH, Immerman EB. Femoral shaft fractures in children: traction and casting versus elastic stable intramedullary nailing. J Trauma. 2002. 53:914–921.
Article5. Dahl MT, Gulli B, Berg T. Complications of limb lengthening. A learning curve. Clin Orthop Relat Res. 1994. 301:10–18.
Article6. Evanoff M, Strong ML, MacIntosh R. External fixation maintained until fracture consolidation in the skeletally immature. J Pediatr Orthop. 1993. 13:98–101.
Article7. Flynn JM, Hresko T, Reynolds RA, Blasier RD, Davidson R, Kasser J. Titanium elastic nails for pediatric femur fractures: a multicenter study of early results with analysis of complications. J Pediatr Orthop. 2001. 21:4–8.
Article8. Flynn JM, Luedtke LM, Ganley TJ, et al. Comparison of titanium elastic nails with traction and a spica cast to treat femoral fractures in children. J Bone Joint Surg Am. 2004. 86:770–777.
Article9. Gregory P, Pevny T, Teague D. Early complications with external fixation of pediatric femoral shaft fractures. J Orthop Trauma. 1996. 10:191–198.
Article10. Gwyn DT, Olney BW, Dart BR, Czuwala PJ. Rotational control of various pediatric femur fractures stabilized with titanium elastic intramedullary nails. J Pediatr Orthop. 2004. 24:172–177.
Article11. Lee SS, Mahar AT, Newton PO. Ender nail fixation of pediatric femur fractures: a biomechanical analysis. J Pediatr Orthop. 2001. 21:442–445.
Article12. Ligier JN, Metaizeau JP, Prévot J, Lascombes P. Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br. 1988. 70:74–77.
Article13. Linhart WE, Roposch A. Elastic stable intramedullary nailing for unstable femoral fractures in children: preliminary results of a new method. J Trauma. 1999. 47:372–378.14. Luhmann SJ, Schootman M, Schoenecker PL, Dobbs MB, Gordon JE. Complications of titanium elastic nails for pediatric femoral shaft fractures. J Pediatr Orthop. 2003. 23:443–447.
Article15. Matzkin EG, Smith EL, Wilson A, Murray PC. External fixation of pediatric femur fractures with cortical contact. Am J Orthop. 2006. 35:498–501.16. Miner T, Carroll KL. Outcomes of external fixation of pediatric femoral shaft fractures. J Pediatr Orthop. 2000. 20:405–410.
Article17. Moroz LA, Launay F, Kocher MS, et al. Titanium elastic nailing of fractures of the femur in children. Predictors of complications and poor outcome. J Bone Joint Surg Br. 2006. 88:1361–1366.18. Simanovsky N, Porat S, Simanovsky N, Eylon S. Close reduction and intramedullary flexible titanium nails fixation of femoral shaft fractures in children under 5 years of age. J Pediatr Orthop B. 2006. 15:293–297.
Article19. Sink EL, Gralla J, Repine M. Complications of pediatric femur fractures treated with titanium elastic nails: a comparison of fracture types. J Pediatr Orthop. 2005. 25:577–580.20. Song HR, Oh CW, Shin HD, et al. Treatment of femoral shaft fractures in young children: comparison between conservative treatment and retrograde flexible nailing. J Pediatr Orthop B. 2004. 13:275–280.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Flexible Intramedullary Nailing with External Fixation in Pediatric Femoral Shaft Fractures
- A Comparison of Overgrowth after Treatment for Pediatric Femoral Shaft Fractures: Flexible Intramedullary Nailing versus External Fixation
- Treatment of Open Type-III Tibial Shaft Fractures -Comparison Between Ilizarov External Fixation and Secondary Intramedullary Nailing-
- Flexible Intramedullary Nail Fixation of Pediatric Femoral Shaft Fracture
- Interlocking Intramedullary Nailing for the Femoral Shaft Fractures
