Comparison of Results of Total Knee Arthroplasty Performed Using the Navigation System and the Conventional Technique: Minimal Follow-Up of 5 Years
- Affiliations
-
- 1Department of Orthopaedic Surgery, Center for Joint Disease, Chonnam National University Hwasun Hospital, Hwasun, Korea. eksong@chonnam.ac.kr
- KMID: 2185318
- DOI: http://doi.org/10.4055/jkoa.2012.47.5.344
Abstract
- PURPOSE
Authors compared the laxity, radiologic and clinical outcomes of total knee arthroplasty (TKA) performed using the navigation system and using the conventional technique at least 5-year follow-up.
MATERIALS AND METHODS
Total of 92 TKAs were included for this study. Forty seven TKAs were performed by the navigation group and 45 TKAs were performed by the conventional surgery. At the final follow up, to evaluate knee joint laxity, varus-valgus laxities were measured on the stress radiographs taken with varus or valgus loads at 90degrees of flexion. The radiologic measurements and the clinical evaluations were compared between two groups.
RESULTS
At the final follow-up, the mean of valgus laxities were 3.9degrees in the navigation group and 4.0degrees in the conventional group, and the corresponding mean of varus laxities were 4.0degrees and 4.3degrees (p=0.19, p=0.22) at 90degrees flexion state. Although there was no significant difference in the total laxities (7.8degrees in the navigation group and 8.1degrees in the conventional group, p=0.35). However, more than 10degrees of total laxity was significantly reduced in the navigation group (1 knee in the navigation group and 6 knees in the conventional group, p=0.04). The outlier numbers at mechanical axis, the mean of coronal inclination of the femoral and tibial component and the mean of sagittal inclination of the femoral and tibial component in the two groups were significantly different. Stiffness of WOMAC score was significantly better in the navigation than in the conventional group (p<0.001).
CONCLUSION
Varus-valgus laxity was significantly different in the two groups as were the outlier numbers. The navigation system could provide good, improved alignment accuracy of the lower extremity and better result in stiffness of knee compared with conventional technique.
Keyword
Figure
-
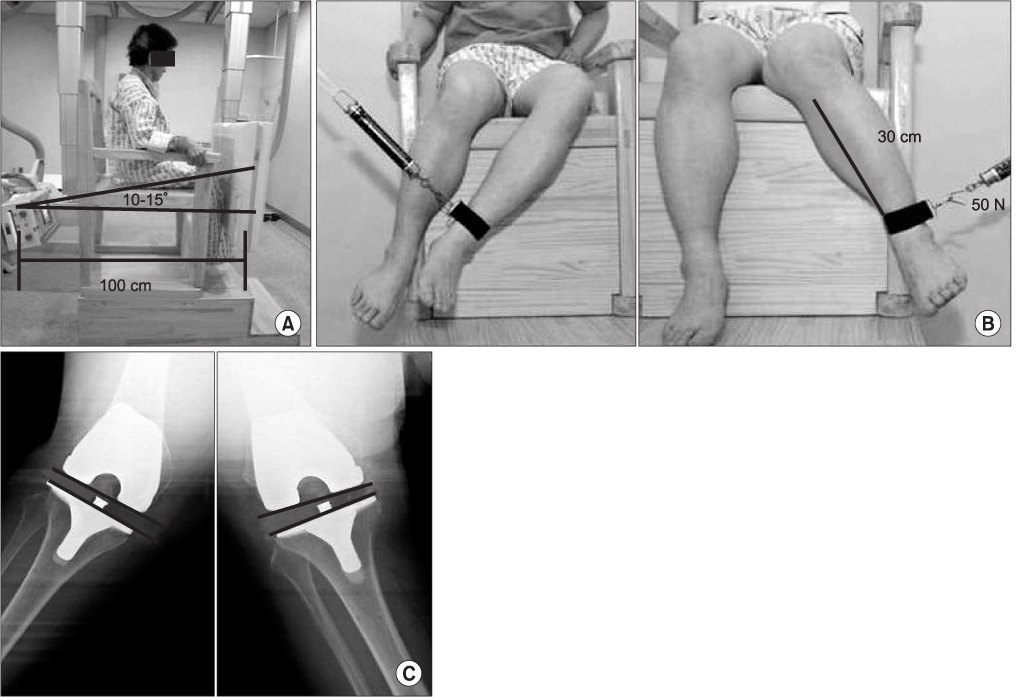
Figure 1 (A) The patients sat on a radiolucent wooden table with their legs hanging over the edge, the knee flexed at 90° with relaxed muscles and touching the vertical cassette stand. The central X-ray beam was aimed from behind the sitting patient in an upward angle of 10-15° into the center of the patella with a film-focus distance of one meter. (B) Valgus or varus force with spring scale (50 N) at 30 cm distal from joint was induced. (C) The joint opening angle between a tangent to the distal femoral condyles and a line between medial and lateral tibial plateaus was measured.

Figure 2 The mechanical axis (θ) of leg is the angle formed between the femoral axis and tibial axis. A (white line), femoral axis; B (black line), tibial axis.
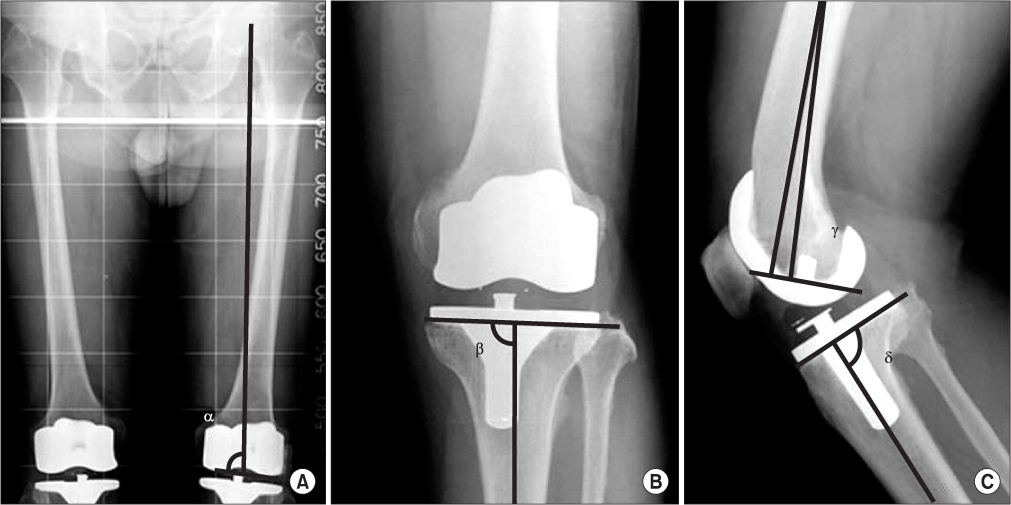
Figure 3 Postoperative measurement of the femoral and tibial components. (A) α: The inclination angle of the femoral component was formed with the mechanical axis of the femur. (B) β: The inclination angle of the tibial component was formed with the mechanical axis of the tibia. (C) γ: The angle of the femoral component was formed between the anatomical axis of the femur and perpendicular line to the prosthesis. δ: The angle of the tibial component was formed with the mechanical axis of the tibia.
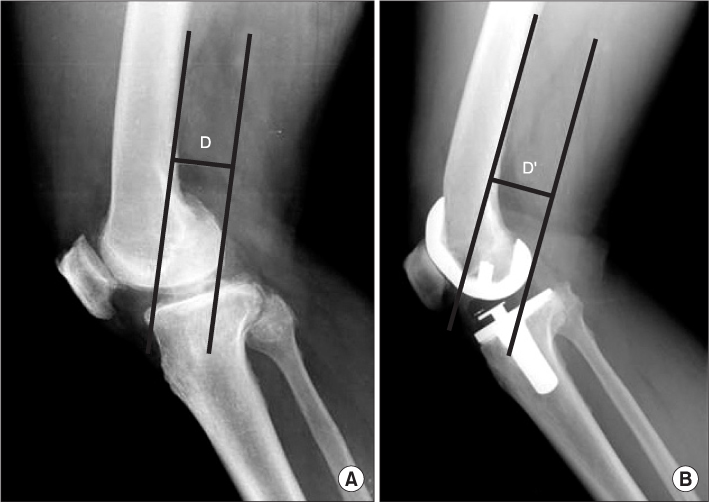
Figure 4 (A) Posterior femoral offset D was defined as the distance between the posterior femoral cortical margin and the posterior margins of the femoral condyles. (B) Postoperative posterior femoral offset D' was defined as the distance between the posterior femoral margin and the posterior margins of the femoral implant condyles.
Reference
-
1. Freeman MA, Todd RC, Bamert P, Day WH. ICLH arthroplasty of the knee: 1968--1977. J Bone Joint Surg Br. 1978. 60:339–344.
Article2. Insall JN, Binazzi R, Soudry M, Mestriner LA. Total knee arthroplasty. Clin Orthop Relat Res. 1985. 192:13–22.
Article3. Stulberg SD, Yaffe MA, Koo SS. Computer-assisted surgery versus manual total knee arthroplasty: a case-controlled study. J Bone Joint Surg Am. 2006. 88:Suppl 4. 47–54.
Article4. Saragaglia D, Picard F, Chaussard C, Montbarbon E, Leitner F, Cinquin P. Computer-assisted knee arthroplasty: comparison with a conventional procedure. Results of 50 cases in a prospective randomized study. Rev Chir Orthop Reparatrice Appar Mot. 2001. 87:18–28.5. Clemens U, Miehlke RK. Experience using the latest Ortho-Pilot TKA software: a comparative study. Surg Technol Int. 2003. 11:265–273.6. Anderson KC, Buehler KC, Markel DC. Computer assisted navigation in total knee arthroplasty: comparison with conventional methods. J Arthroplasty. 2005. 20:7 Suppl 3. 132–138.7. Bäthis H, Perlick L, Tingart M, Lüring C, Zurakowski D, Grifka J. Alignment in total knee arthroplasty. A comparison of computer-assisted surgery with the conventional technique. J Bone Joint Surg Br. 2004. 86:682–687.8. Song EK, Seon JK, Chung JY, Cho SG, Kong IK. Comparison of results of total knee arthroplasty performed using a navigation system and the conventional technique. J Korean Orthop Assoc. 2006. 41:1002–1007.
Article9. Pierson JL, Ritter MA, Keating EM, et al. The effect of stuffing the patellofemoral compartment on the outcome of total knee arthroplasty. J Bone Joint Surg Am. 2007. 89:2195–2203.
Article10. Ewald FC. The Knee Society total knee arthroplasty roentgenographic evaluation and scoring system. Clin Orthop Relat Res. 1989. 248:9–12.
Article11. Bellamy N. Pain assessment in osteoarthritis: experience with the WOMAC osteoarthritis index. Semin Arthritis Rheum. 1989. 18:4 Suppl 2. 14–17.
Article12. Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res. 1989. 248:13–14.
Article13. Haaker RG, Stockheim M, Kamp M, Proff G, Breitenfelder J, Ottersbach A. Computer-assisted navigation increases precision of component placement in total knee arthroplasty. Clin Orthop Relat Res. 2005. 433:152–159.
Article14. Heesterbeek PJ, Keijsers NL, Wymenga AB. Ligament releases do not lead to increased postoperative varus-valgus laxity in flexion and extension: a prospective clinical study in 49 TKR patients. Knee Surg Sports Traumatol Arthrosc. 2010. 18:187–193.
Article15. Worland RL, Jessup DE, Johnson J. Posterior cruciate recession in total knee arthroplasty. J Arthroplasty. 1997. 12:70–73.
Article16. Pang HN, Yeo SJ, Chong HC, Chin PL, Ong J, Lo NN. Computer-assisted gap balancing technique improves outcome in total knee arthroplasty, compared with conventional measured resection technique. Knee Surg Sports Traumatol Arthrosc. 2011. 19:1496–1503.
Article17. Cheng T, Zhao S, Peng X, Zhang X. Does computer-assisted surgery improve postoperative leg alignment and implant positioning following total knee arthroplasty? A meta-analysis of randomized controlled trials? Knee Surg Sports Traumatol Arthrosc. 2012. 20:1307–1322.
Article18. Bellemans J, Banks S, Victor J, Vandenneucker H, Moemans A. Fluoroscopic analysis of the kinematics of deep flexion in total knee arthroplasty. Influence of posterior condylar offset. J Bone Joint Surg Br. 2002. 84:50–53.19. Massin P, Gournay A. Optimization of the posterior condylar offset, tibial slope, and condylar roll-back in total knee arthroplasty. J Arthroplasty. 2006. 21:889–896.
Article20. Goldstein WM, Raab DJ, Gleason TF, Branson JJ, Berland K. Why posterior cruciate-retaining and substituting total knee replacements have similar ranges of motion. The importance of posterior condylar offset and cleanout of posterior condylar space. J Bone Joint Surg Am. 2006. 88:Suppl 4. 182–188.21. McEwen HM, Barnett PI, Bell CJ, et al. The influence of design, materials and kinematics on the in vitro wear of total knee replacements. J Biomech. 2005. 38:357–365.
Article22. O'Rourke MR, Callaghan JJ, Goetz DD, Sullivan PM, Johnston RC. Osteolysis associated with a cemented modular posterior-cruciate-substituting total knee design: five to eight-year follow-up. J Bone Joint Surg Am. 2002. 84:1362–1371.23. Lachiewicz PF, Soileau ES. The rates of osteolysis and loosening associated with a modular posterior stabilized knee replacement. Results at five to fourteen years. J Bone Joint Surg Am. 2004. 86:525–530.24. Ishida K, Matsumoto T, Tsumura N, et al. Mid-term outcomes of computer-assisted total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2011. 19:1107–1112.
Article25. Brander VA, Stulberg SD, Adams A, Wood O. CAS-TKA reduces the occurrence of functional outliers. Paper presented at: Fourth Annual Meeting of CAOS International. June 16-19, 2004; Chicago.26. Lützner J, Günther KP, Kirschner S. Functional outcome after computer-assisted versus conventional total knee arthroplasty:a randomized controlled study. Knee Surg Sports Traumatol Arthrosc. 2010. 18:1339–1344.27. Kamat YD, Aurakzai KM, Adhikari AR, Matthews D, Kalairajah Y, Field RE. Does computer navigation in total knee arthroplasty improve patient outcome at midterm follow-up? Int Orthop. 2009. 33:1567–1570.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Results of Total Knee Arthroplasty Performed using a Navigation System and the Conventional Technique
- Comparison of an Accelerometer-Based Portable Navigation System, Patient-Specific Instrumentation, and Conventional Instrumentation for Femoral Alignment in Total Knee Arthroplasty
- Computer-Assisted Navigation in Total Knee Arthroplasty
- Accuracy of Limb Alignment in Total Knee Arthroplasty using Image-Free Navigation System: Comparison with Conventional Total Knee Arthroplasty
- Effects of Femoral Lateral Bowing on Coronal Alignment and Component Position after Total Knee Arthroplasty: A Comparison of Conventional and Navigation-Assisted Surgery
