Non-Hodgkin Lymphoma Occurred in Psoas Muscle
- Affiliations
-
- 1Department of Orthopedic Surgery, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea. oskim@paik.ac.kr
- KMID: 2185286
- DOI: http://doi.org/10.4055/jkoa.2013.48.6.486
Abstract
- One fourth of cases of non-Hodgkin lymphoma were reported as extranodal type and skeletal muscle involvement rarely seen as a primary event and local dissemination. The psoas involved lesion with spine mimicking pain is caused mainly by infection rather than non-infected conditions such as tumor. We report on a rare case of non-Hodgkin lymphoma occurring in psoas muscle, which required differentiation from a psoas abscess.
Keyword
Figure
-

Figure 1 Preoperative magnetic resonance imaging findings. (A) Herniated nucleus pulposus of T12-L1 in sagittal view. (B) Axial view of T12-L1: Right dominant central protruding disc.
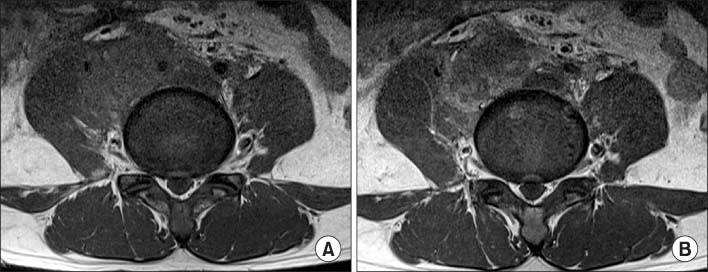
Figure 2 Preoperative magnetic resonance imaging findings. (A) Irregular heterogenous mass in right psoas muscle region in axial view. (B) Peripheral enhancing mass that invades right psoas muscle.

Figure 3 Preoperative positron emission tomography findings. (A) Peripheral fluorodeoxyglucose (FDG) uptake along the right psoas muscle in coronal view. (B) Central necrosis and peripheral strong FDG uptake in right psoas muscle in axial view.
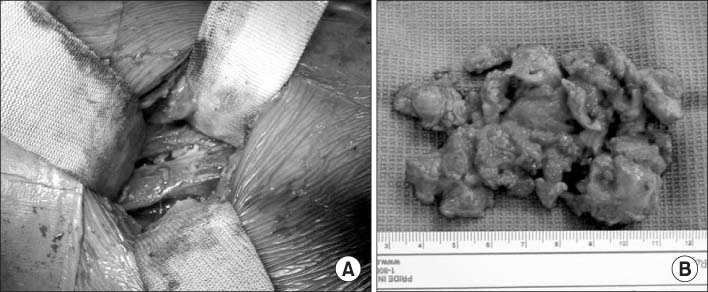
Figure 4 Intraoperative picture and removed necrotic mass. (A) Irregular mass with necrotic tissue in right psoar muscle. (B) Removed necrotic mass.
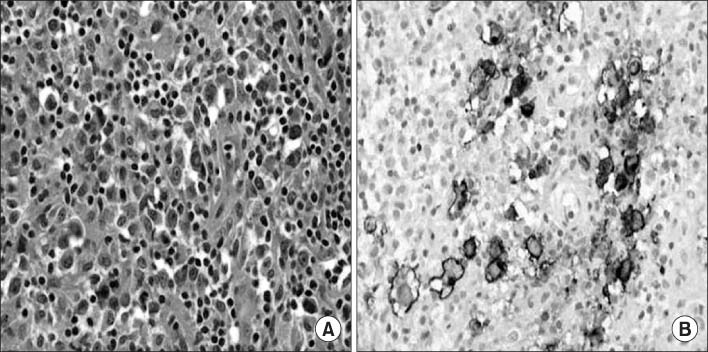
Figure 5 Pathologic findings. (A) Diffuse infiltration of malignant cells, some showing Reed-Sternberg like features (H&E, ×400). (B) Immunohistochemical stain for CD30 was positive in the larger neoplastic cells (×400).
Reference
-
1. Ishii E, Honda K, Nakagawa A, Urago K, Oshima K. Primary CD30/Ki-1 positive anaplastic large cell lymphoma of skeletal muscle with der(17)t(1;17)(q11;p11). Cancer Genet Cytogenet. 2000; 122:116–120.
Article2. Chim CS, Loong F, Ooi GC, Srivastava G, Liang R. Primary skeletal muscle lymphoma. Am J Med. 2002; 112:79–80.
Article3. Glass AG, Karnell LH, Menck HR. The National Cancer Data Base report on non-Hodgkin's lymphoma. Cancer. 1997; 80:2311–2320.
Article4. Ueno A, Kuribayashi K, Iyama S, et al. Two cases of primary skeletal muscle lymphoma, and a review of the literature. Rinsho Ketsueki. 2005; 46:1141–1145.5. Masaoka S, Fu T. Malignant lymphoma in skeletal muscle with rhabdomyolysis: a report of two cases. J Orthop Sci. 2002; 7:688–693.
Article6. Kim YM, Won CH, Seo JB, Choi ES, Lee HS, Um SM. Pyogenic L4-5 spondylitis managed with percutaneous drainage followed by posterior lumbar interbody fusion: a case report. J Korean Soc Spine Surg. 2001; 8:513–519.7. Mückley T, Schütz T, Kirschner M, Potulski M, Hofmann G, Bühren V. Psoas abscess: the spine as a primary source of infection. Spine (Phila Pa 1976). 2003; 28:E106–E113.
Article8. Kounami S, Shibuta K, Yoshiyama M, et al. Primary anaplastic large cell lymphoma of the psoas muscle: a case report and literature review. Acta Haematol. 2012; 127:186–188.
Article
