J Korean Orthop Assoc.
2014 Aug;49(4):316-320. 10.4055/jkoa.2014.49.4.316.
A Case of Gait Disturbance due to Chronic Bilateral Subdural Hematoma Mimicking Cervical Spondylotic Myelopathy
- Affiliations
-
- 1Department of Orthopaedic Surgery, Chonbuk National University Medical School, Jeonju, Korea.
- 2Department of Orthopaedic Surgery, St. Carollo Hospital, Suncheon, Korea. osman2008@naver.com
- KMID: 2185194
- DOI: http://doi.org/10.4055/jkoa.2014.49.4.316
Abstract
- Cervical spondylotic myelopathy (CSM) is a spinal cord dysfunction involving compression of the vascular and neural structures due to bony spurring or soft tissue hypertrophy in patients with degenerative cervical disorders. It presents initially as subtle gait disturbance with gradual deterioration. An elderly patient presenting with gait disturbance due to spasticity and motor weakness of both lower extremities without mental change can be easily misdiagnosed as CSM. We report on a case of gait disturbance due to chronic bilateral subdural hematoma mimicking CSM.
MeSH Terms
Figure
-
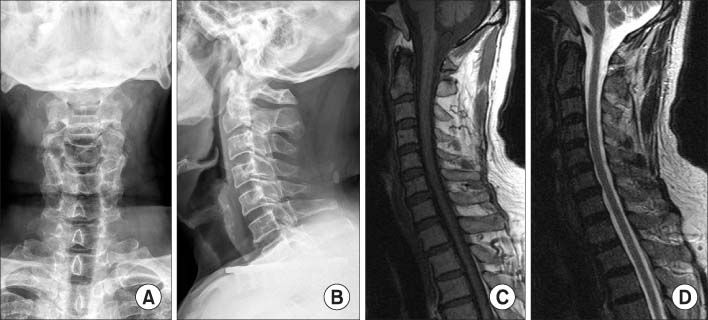
Figure 1 (A, B) Cervical radiographs. (C, D) Magnetic resonance images (T1 and T2 sagittal).
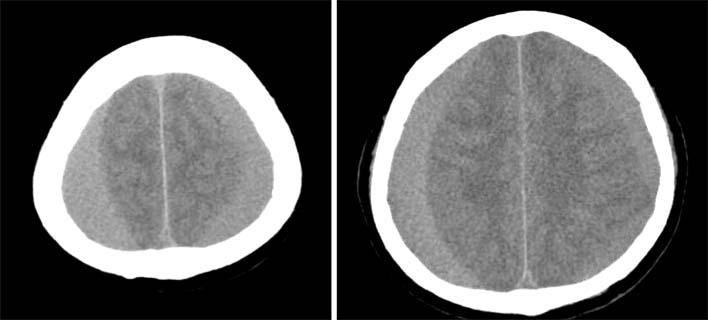
Figure 2 Non-enhanced brain computed tomography scan showing slightly high- or iso-density of the bilateral chronic subdural hematoma, larger on the right.
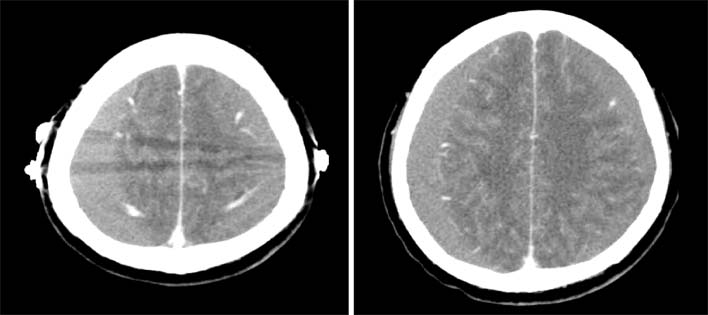
Figure 3 Preoperative enhanced computed tomography scan showing markers on the parietal eminence for the perforating point.
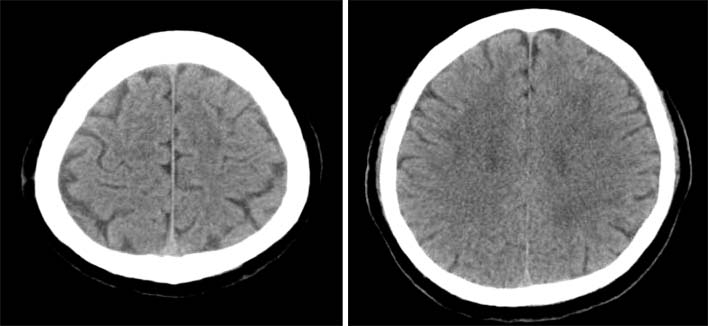
Figure 4 Postoperative computed tomography scan; one month after surgery, complete drainage of the hematoma and expansion of the bilateral hemisphere.
Reference
-
1. Song KJ, Choi BW, Park HJ. Anterior cervical decompression and fusion for the treatment of cervical spondylotic myelopathy. J Korean Orthop Assoc. 2002; 37:787–794.
Article2. Mikawa Y, Shikata J, Yamamuro T. Spinal deformity and instability after multilevel cervical laminectomy. Spine (Phila Pa 1976). 1987; 12:6–11.
Article3. Okada Y, Akai T, Okamoto K, Iida T, Takata H, Iizuka H. A comparative study of the treatment of chronic subdural hematoma--burr hole drainage versus burr hole irrigation. Surg Neurol. 2002; 57:405–409.
Article4. Ko BS, Lee JK, Seo BR, Moon SJ, Kim JH, Kim SH. Clinical analysis of risk factors related to recurrent chronic subdural hematoma. J Korean Neurosurg Soc. 2008; 43:11–15.
Article5. Frati A, Salvati M, Mainiero F, et al. Inflammation markers and risk factors for recurrence in 35 patients with a posttraumatic chronic subdural hematoma: a prospective study. J Neurosurg. 2004; 100:24–32.
Article6. Choi WW, Kim KH. Prognostic factors of chronic subdural hematoma. J Korean Neurosurg Soc. 2002; 32:18–22.7. McLachlan RS, Bolton CF, Coates RK, Barnett HJ. Gait disturbance in chronic subdural hematoma. Can Med Assoc J. 1981; 125:865–868.8. Suman S, Meenakshisundaram S, Woodhouse P. Bilateral chronic subdural haematoma: a reversible cause of parkinsonism. J R Soc Med. 2006; 99:91–92.
Article9. Rao R. Neck pain, cervical radiculopathy, and cervical myelopathy: pathophysiology, natural history, and clinical evaluation. J Bone Joint Surg Am. 2002; 84:1872–1881.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bilateral Acute Subdural Hematoma Following Evacuation of Chronic Subdural Hematoma
- Intraoperative Development of Contralateral Subdural Hematoma during Evacuation of Acute Subdural Hematoma: Case Report
- Chronic Subdural Hematoma Superimposed on Posttraumatic Subdural Hygroma: A Report of Three Cases
- Multi-Layer Chronic Subdural Hematoma Requiring Craniotomy
- A Case of Aggravated Chronic Subdural Hematoma after Cervical Myelography
