Endoprosthetic Reconstruction in the Limb Salvage Surgery for Treatment of Malignant Bone Tumors
- Affiliations
-
- 1Department of Orthopaedic Surgery, Seoul National University Hospital, Seoul, Korea. hankim@snu.ac.kr
- KMID: 2185086
- DOI: http://doi.org/10.4055/jkoa.2015.50.6.453
Abstract
- Endoprosthetic replacement is the most frequently used surgical method for the skeletal reconstruction in the limb salvage surgery for malignant bone tumors. Modular prostheses are generally used for typical locations such as distal and proximal femur, proximal tibia and proximal humerus. Expandable prosthesis is used to overcome leg length discrepancy in growing children. Aseptic loosening, infection and mechanical failure are major complications resulting in revision surgery. Many efforts should be made to develop more durable and functional implants to improve the quality of life of sarcoma survivors.
MeSH Terms
Figure
-

Figure 1 Osteosarcoma of the distal femur. (A) Osteolytic lesion of the medullary canal and periosteal reaction are seen on the plain radiograph. (B) Intramedullary geographic lesion of low signal is seen on the T1 weighted magnetic resonance imaging. (C) The image shows endoprosthetic replacement with uncemented fixation of the distal femur.

Figure 2 (A) Plain radiographs show the total femur replacement with bipolar type. (B) Photograph of the total femoral prosthesis with expandable type.
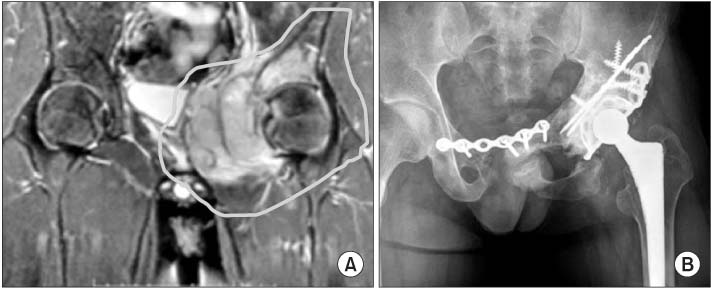
Figure 3 Osteosarcoma of the pelvis. (A) The tumor is located in the superior ramus and acetabulum with huge extraosseous mass formation, which suggests osteosarcoma of the pelvis. (B) After type II, III pelvic resection, which means resection of pubic ramus (type III) and acetabulum (type II), hip was reconstructed with pelvic allograft (for acetabulum) augmented with reinforcement cage and cemented fixation. The allograft with cage was fixed with ilium using pins, plate and screws. The junction between the ilium and the acetabulum of the allograft was well united.

Figure 4 Expandable prosthesis of the distal femur. (A) After resection of the distal femur, custom type expandable prosthesis was placed with cement fixation. (B) Screwdriver pits for lengthening procedure are seen at the proximal portion of the implant. (C) After two times of lengthening procedure, the length of 4 cm was gained.
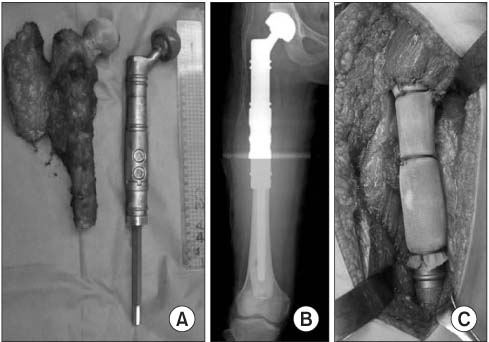
Figure 5 Modular-type endoprosthesis of the proximal femur. (A) During the operation, a surgeon can select the implant of the same size with the excised specimen. (B) Plain radiograph shows the well placed implant instead of the proximal femur. (C) The implant is wrapped tightly with the fabric-like polymer material, and the hip abductors and psoas muscle were sutured to the material.
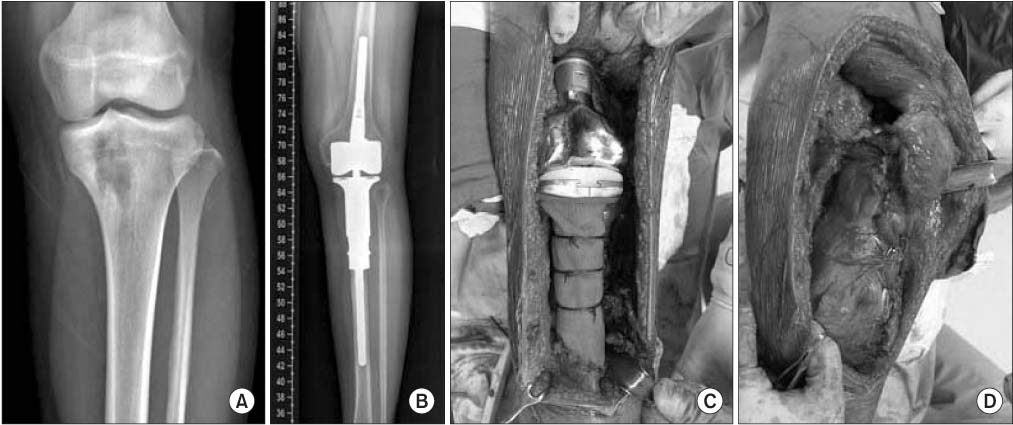
Figure 6 Endoprosthesis of the proximal tibia. (A) Osteosarcoma of the proximal tibia. (B) Endoprosthesis was placed after excision of the proximal tibial lesion. (C) The implant is wrapped tightly with the fabric-like polymer material for attachment of the patellar tendon. (D) The implant was covered with the muscle flap in order not to be placed just beneath the skin.
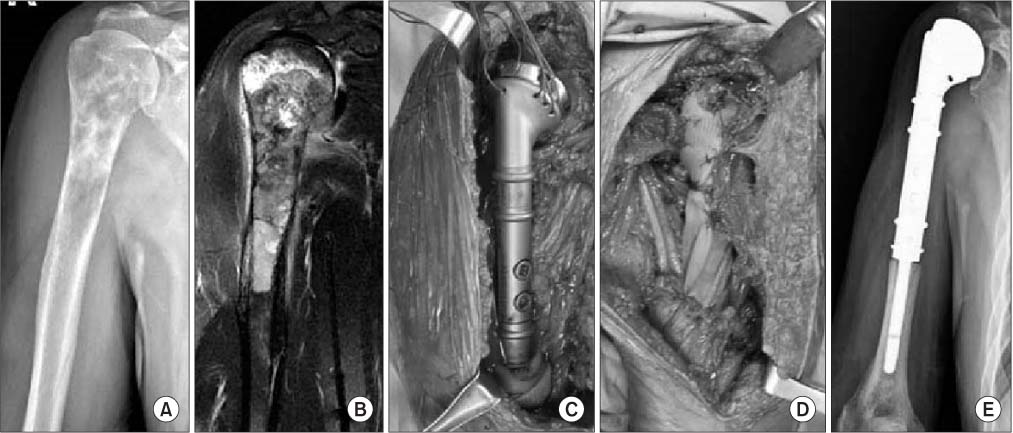
Figure 7 Endoprosthetic replacement for the proximal humerus. (A) A typical image of the proximal humeral osteosarcoma. (B) The magnetic resonance imaging finding is compatible with the osteosarcoma. (C) A photograph of the endoprosthesis. (D) Surrounding muscles are attached the polymer material wrapped around the implant. (E) Postoperative radiograph.
Reference
-
1. Sim FH, Chao EY. Prosthetic replacement of the knee and a large segment of the femur or tibia. J Bone Joint Surg Am. 1979; 61:887–892.
Article2. Roberts P, Chan D, Grimer RJ, Sneath RS, Scales JT. Prosthetic replacement of the distal femur for primary bone tumours. J Bone Joint Surg Br. 1991; 73:762–769.
Article3. Kotz R, Ritschl P, Trachtenbrodt J. A modular femur-tibia reconstruction system. Orthopedics. 1986; 9:1639–1652.
Article4. Lewis MM, Bloom N, Esquieres EM, Kenan S, Ryniker DM. The expandable prosthesis. An alternative to amputation for children with malignant bone tumors. AORN J. 1987; 46:457–470.5. Han I, Lee SH, Cho HS, Oh JH, Kim HS. Use of expandable prostheses in malignant bone tumors in children. J Korean Bone Joint Tumor Soc. 2008; 14:10–16.6. Abudu A, Grimer R, Tillman R, Carter S. The use of prostheses in skeletally immature patients. Orthop Clin North Am. 2006; 37:75–84.
Article7. Nystrom LM, Morcuende JA. Expanding endoprosthesis for pediatric musculoskeletal malignancy: current concepts and results. Iowa Orthop J. 2010; 30:141–149.8. Raiss P, Kinkel S, Sauter U, Bruckner T, Lehner B. Replacement of the proximal humerus with MUTARS tumor endoprostheses. Eur J Surg Oncol. 2010; 36:371–377.
Article9. King JJ, Nystrom LM, Reimer NB, Gibbs CP Jr, Scarborough MT, Wright TW. Allograft-prosthetic composite reverse total shoulder arthroplasty for reconstruction of proximal humerus tumor resections. J Shoulder Elbow Surg. 2015; 08. 06. Published online. DOI: 10.1016/j.jse.2015.06.021.
Article10. Capanna R, Scoccianti G, Frenos F, Vilardi A, Beltrami G, Campanacci DA. What was the survival of megaprostheses in lower limb reconstructions after tumor resections? Clin Orthop Relat Res. 2015; 473:820–830.
Article11. Kim HS, Kim KJ, Han I, Oh JH, Lee SH. The use of pasteurized autologous grafts for periacetabular reconstruction. Clin Orthop Relat Res. 2007; 464:217–223.
Article12. Capanna R, Morris HG, Campanacci D, Del Ben M, Campanacci M. Modular uncemented prosthetic reconstruction after resection of tumours of the distal femur. J Bone Joint Surg Br. 1994; 76:178–186.
Article13. Flint MN, Griffin AM, Bell RS, Ferguson PC, Wunder JS. Aseptic loosening is uncommon with uncemented proximal tibia tumor prostheses. Clin Orthop Relat Res. 2006; 450:52–59.
Article14. Pala E, Trovarelli G, Calabrò T, Angelini A, Abati CN, Ruggieri P. Survival of modern knee tumor megaprostheses: failures, functional results, and a comparative statistical analysis. Clin Orthop Relat Res. 2015; 473:891–899.
Article15. Palumbo BT, Henderson ER, Groundland JS, et al. Advances in segmental endoprosthetic reconstruction for extremity tumors: a review of contemporary designs and techniques. Cancer Control. 2011; 18:160–170.
Article16. Hardes J, von Eiff C, Streitbuerger A, et al. Reduction of periprosthetic infection with silver-coated megaprostheses in patients with bone sarcoma. J Surg Oncol. 2010; 101:389–395.
Article17. Chandrasekar CR, Grimer RJ, Carter SR, Tillman RM, Abudu A, Buckley L. Modular endoprosthetic replacement for tumours of the proximal femur. J Bone Joint Surg Br. 2009; 91:108–112.
Article18. Bernthal NM, Greenberg M, Heberer K, Eckardt JJ, Fowler EG. What are the functional outcomes of endoprosthestic reconstructions after tumor resection? Clin Orthop Relat Res. 2015; 473:812–819.
Article19. Menendez LR, Ahlmann ER, Kermani C, Gotha H. Endoprosthetic reconstruction for neoplasms of the proximal femur. Clin Orthop Relat Res. 2006; 450:46–51.
Article20. Houdek MT, Wagner ER, Wilke BK, Wyles CC, Taunton MJ, Sim FH. Long term outcomes of cemented endoprosthetic reconstruction for periarticular tumors of the distal femur. Knee. 2015; 09. 08. Published online. DOI: 10.1016/j.knee.2015.08.010.
Article21. Malawer MM, Chou LB. Prosthetic survival and clinical results with use of large-segment replacements in the treatment of high-grade bone sarcomas. J Bone Joint Surg Am. 1995; 77:1154–1165.
Article22. Bergin PF, Noveau JB, Jelinek JS, Henshaw RM. Aseptic loosening rates in distal femoral endoprostheses: does stem size matter? . Clin Orthop Relat Res. 2012; 470:743–750.
Article23. Kawai A, Backus SI, Otis JC, Healey JH. Interrelationships of clinical outcome, length of resection, and energy cost of walking after prosthetic knee replacement following resection of a malignant tumor of the distal aspect of the femur. J Bone Joint Surg Am. 1998; 80:822–831.
Article24. Puchner SE, Kutscha-Lissberg P, Kaider A, et al. Outcome after reconstruction of the proximal tibia: complications and competing risk analysis. PLoS One. 2015; 10:e0135736.25. Lee SH, Kim HS, Park YB, Rhie TY, Lee HK. Prosthetic reconstruction for tumours of the distal tibia and fibula. J Bone Joint Surg Br. 1999; 81:803–807.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of malignant bone tumor: limb salvage surgery using metallic tumor prosthesis
- Treatment of Malignant Bone Tumors by Tumor Prosthesis
- The Primary Malignant Bone Tumors of Distal Tibia: Comparison between Limb Salvage and Amputation
- Recent Advances in Malignant Bone Tumor Treatment
- Limb Salvage with Low and Heat Treated Autobone
