Surgical Resection of Malignant Bone Tumors
- Affiliations
-
- 1Department of Orthopedic Surgery, Chonnam National University Medical School, Gwangju, Korea. stjung@chonnam.ac.kr
- KMID: 2185085
- DOI: http://doi.org/10.4055/jkoa.2015.50.6.444
Abstract
- Malignant bone tumors are less common than other tumors, and we often make a misdiagnosis. However, due to its severity and prognosis we should not pass over the malignant bone tumor, because it is one of the important diseases to diagnose. Specific techniques are available for the resection and reconstruction of malignant bone tumors from the body involving extremities. In particular, it is necessary to establish guidelines for elimination of tumor cells as much as possible and minimize the malfunction. Knowledge of the staging system and guide lines for resection margin is required for treatment of malignant bone tumors.
Keyword
Figure
-
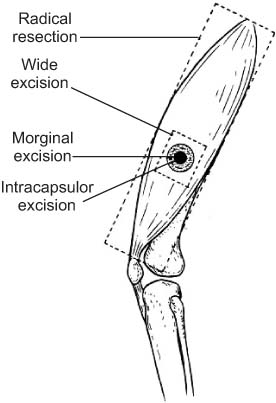
Figure 1 Surgical margin. Cited from the article of Enneking (Instr Course Lect. 1988;37:3-10)10) with original copyright holder's permission.

Figure 2 Surgical margin from Kawaguchi. The principle of curative wide resection is that, when a barrier exists, the tumor is removed outside the barrier. When a barrier is not present, the tumor is removed using as much margin as possible greater than 5 cm. (A) In case of a skin or subcutaneous lesion, the lesion is removed with a margin of 5 cm or more where the barrier does not exist and outside the barrier where it does exist. (B) If the lesion arises in an intermuscular area, the margin is more than 5 cm where there is no barrier. (C) In intramuscular lesions, the muscle surrounding the tumor is removed 5 cm from the reactive zone where a barrier does not exist, and the dissection and resection of the nearby tissues depends on the barrier rather than the true physical distance from the lesion. (D) In bone sarcoma, the tumor is removed 5 cm from the lesion if a barrier does not exist like the site of the nearby diaphysis of the bone but if a barrier exists the barriers are converted into equivalent distances and the tumor is removed accordingly. Cited from the article by Kawaguchi et al. (Clin Orthop Relat Res. 2004;419:165-72)9) with original copyright holder's permission.

Figure 3 Case 1. (A) A 27-year-old female who underwent planned excision. (A) Preoperative plain radiograph. (B) Coronal, saggital, axial view of the magnetic resonance imaging taken before a planned surgical treatment. (C) Gross clinical photograph of the widely excised tumor. (D) Postoperative plain radiograph.

Figure 4 Case 2. A 15-year-old female who undedrwent planned excision. (A) Preoperative plain radiograph. (B) Coronal, saggital, axial view of the magnetic resonance imaging taken before a planned surgical treatment. (C) Gross clinical photograph of the widely excised tumor. (D) Postoperative plain radiograph.
Reference
-
1. Link MP, Goorin AM, Miser AW, et al. The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med. 1986; 314:1600–1606.2. Bernthal NM, Federman N, Eilber FR, et al. Long-term results (>25 years) of a randomized, prospective clinical trial evaluating chemotherapy in patients with high-grade, operable osteosarcoma. Cancer. 2012; 118:5888–5893.3. Collins M, Wilhelm M, Conyers R, et al. Benefits and adverse events in younger versus older patients receiving neoadjuvant chemotherapy for osteosarcoma: findings from a metaanalysis. J Clin Oncol. 2013; 31:2303–2312.4. Aho AJ, Ekfors T, Dean PB, Aro HT, Ahonen A, Nikkanen V. Incorporation and clinical results of large allografts of the extremities and pelvis. Clin Orthop Relat Res. 1994; 307:200–213.5. Camnasio F, Scotti C, Peretti GM, Fontana F, Fraschini G. Prosthetic joint replacement for long bone metastases: analysis of 154 cases. Arch Orthop Trauma Surg. 2008; 128:787–793.6. Gosheger G, Gebert C, Ahrens H, Streitbuerger A, Winkelmann W, Hardes J. Endoprosthetic reconstruction in 250 patients with sarcoma. Clin Orthop Relat Res. 2006; 450:164–171.7. Edge S, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer-Verlag;2009.8. Enneking WF, Spanier SS, Goodman MA. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res. 1980; 153:106–120.9. Kawaguchi N, Ahmed AR, Matsumoto S, Manabe J, Matsushita Y. The concept of curative margin in surgery for bone and soft tissue sarcoma. Clin Orthop Relat Res. 2004; 419:165–172.10. Enneking WF. A system of staging musculoskeletal neoplasms. Instr Course Lect. 1988; 37:3–10.11. Kawaguchi N, Amino K, Matsumoto S, et al. Limiting factors of limb salvage operation for musculoskeletal sarcoma. In : Yamamuro T, editor. New developments for limb salvage in musculoskeletal tumors. Kyocera Orthopaedic Symposium. Tokyo: Springer-Verlag;1989. p. 137–141.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Malignant Bone Tumors by Tumor Prosthesis
- Recent Advances in Malignant Bone Tumor Treatment
- Reconstruction with Replantation of the Resected Bone after Low Heat Treatment for Malignant Pelvic Bone Tumors
- The Results of Hemicortical Resection for Malignant Bone Tumor
- Reconstruction of Large Bone Defect after Wids Segmental Resection of Long Bone Tumors Using the Free Vascularized Fibular Graft
