J Korean Med Assoc.
2006 Feb;49(2):181-186. 10.5124/jkma.2006.49.2.181.
Aspirin for the Prevention of Cardiovascular Events
- Affiliations
-
- 1Department of Internal Medicine, Ulsan University College of Medicine, Asan Medical Center, Korea. cheolwlee@amc.seoul.kr
- KMID: 2184666
- DOI: http://doi.org/10.5124/jkma.2006.49.2.181
Abstract
- Plaque disruption and subsequent thrombotic occlusion is the primary mechanism by which atherosclerosis leads to acute coronary syndromes and ischemic stroke. Platelets are the key component of arterial thrombus formation in response to sudden fissuring or rupture of the atheromatous plaque. Low dose aspirin (100~300 mg/day) rapidly inhibits platelets through permanent inactivation of the key platelet enzyme, cyclooxygenase (COX). The efficacy and safety of aspirin have been extensively studied in several populations, ranging from healthy individuals to highrisk patients with acute myocardial infarction or ischemic stroke. It is well established that aspirin reduces the risk of serious vascular events (death, myocardial infarction, and stroke) by approximately 25% in patients with established vascular diseases. However, long-term therapy with aspirin approximately doubles the risk of major extracranial bleeding (mostly gastrointestinal bleeding) and also increases the risk of hemorrhagic stroke. In contrast to the clear benefit of aspirin in secondary prevention, its benefits in primary prevention are less clear. A meta-analysis of primary prevention trials in men demonstrated that aspirin reduces the risk of myocardial infarction by approximately 30% but has no effects on the risk of stroke. By contrast, the Women's Health Study showed that aspirin reduces the risk of stroke by 17% but has no effects on the risk of myocardial infarction. The reasons for this discrepancy remain unclear, requiring additional studies. Taken together, aspirin is recommended for primary prevention in healthy individuals with an annual risk of vascular events >1.5%. In conclusion, aspirin is recommended for secondary prevention in all patients, but its risk-benefit ratio should be carefully considered for primary prevention.
Keyword
MeSH Terms
Figure
-
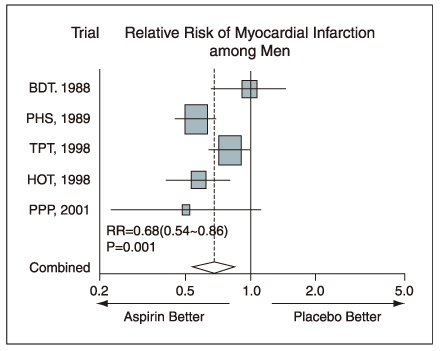
Figure 1 Aspirin for the primary prevention of myocardial infarction

Figure 2 Asprin for stroke prevention
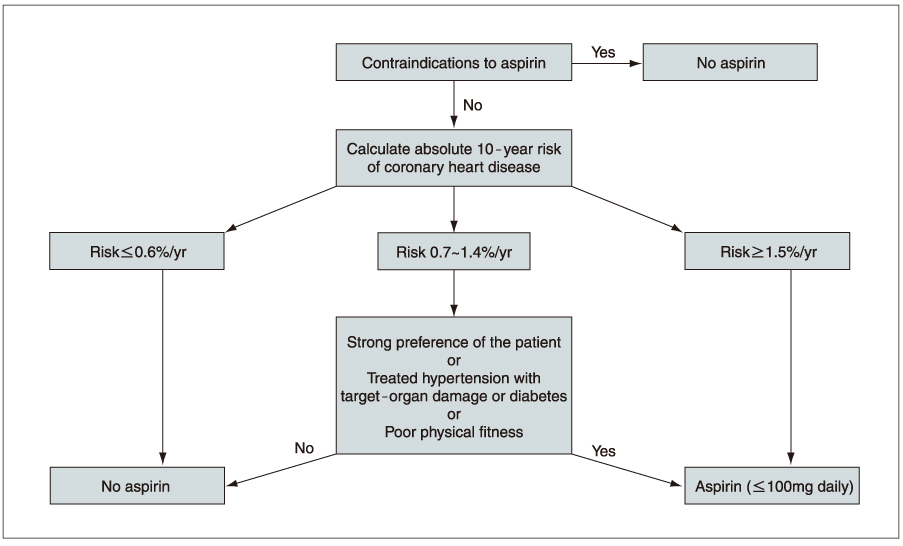
Figure 3 Suggested algorithm for the use of aspirin for primary prevention
Reference
-
1. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005. 352:1685–1695.
Article2. Antithrombotic Trialists' Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high-risk patients. BMJ. 2002. 324:71–78.3. Collaborative Group of the Primary Prevention Project. Low-dose aspirin and vitamin E in people at cardiovascular risk: a randomised trial in general practice. Lancet. 2001. 357:89–95.4. Ridker PM, Cook NR, Lee IM, et al. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N Engl J Med. 2005. 352:1293–1304.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Aspirin for Primary Prevention of Cardiovascular Disease
- The Prevalence of a Low Response to Aspirin and its Association with Recurrent Ischemic Cerebrovascular Events
- Aspirin in the prevention of cardiovascular disease and cancer
- Aspirin Resistance in Patients with End-Stage Renal Disease
- Effects of Antiplatelet Drugs in Cardiovascular Prevention
