Progression of Left Ventricular Pseudoaneurysm after an Acute Myocardial Infarction
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. smparkmd@korea.ac.kr
- KMID: 2177321
- DOI: http://doi.org/10.4250/jcu.2010.18.4.161
Abstract
- Left ventricular (LV) pseudoaneurysms rarely occur, but are detected more often with the development of new diagnostic tools. Since LV pseudoaneurysms are life-threatening, early surgical intervention is recommended. This report describes an 87-year-old woman with heart failure and a large LV pseudoaneurysm which progressed from a small LV pseudoaneurysm after an acute myocardial infarction over a 1-year period.
MeSH Terms
Figure
-
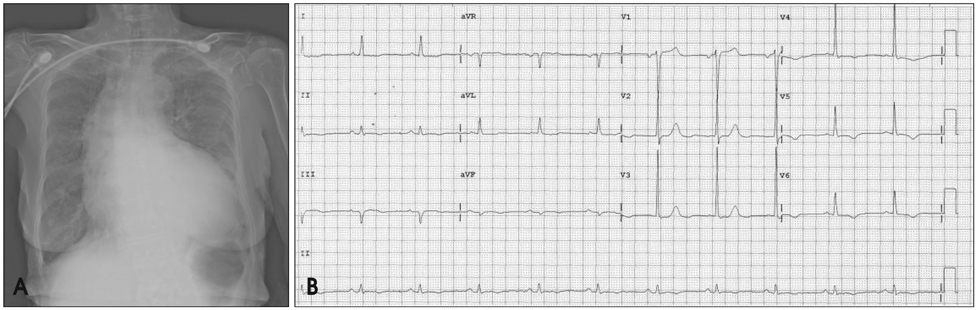
Fig. 1 Chest radiograph (A) shows cardiomegaly with a cardiothoracic ratio of 75%, pulmonary congestion, and a tortuous aorta. The electrocardiography (B) shows voltage criteria of LV hypertrophy and T wave inversion in leads V5 and V6, compatible with LV strain. LV: left ventricle.
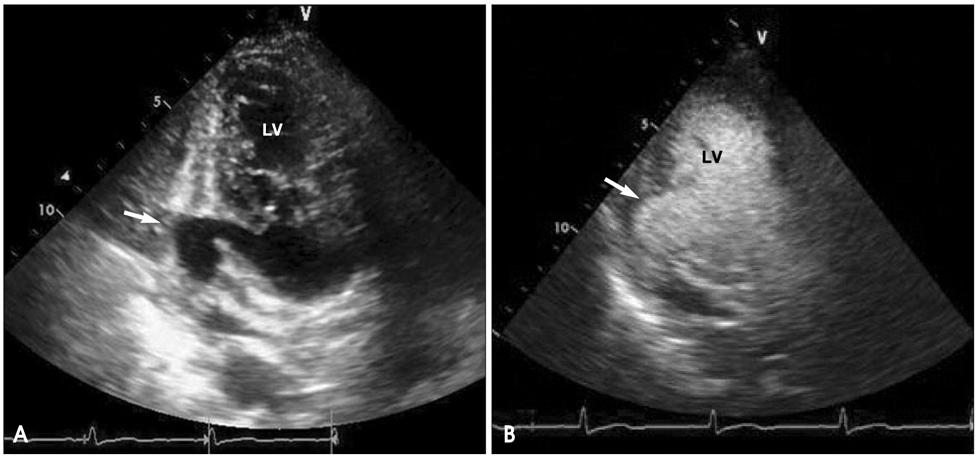
Fig. 2 During the previous admission, transthoracic two-dimensional echocardiography (A) shows an echo-free space (arrow) with a maximal diameter of 22×11 mm and a neck of 15×17 mm. The myocardium at the neck abruptly stops, and a thrombotic plug is observed. Contrast echocardiography (B) shows better margin of the pseudoaneurysm (arrow) and no clear visualization of dye leakage to the pericardial space. LV: left ventricle.

Fig. 3 Cardiac magnetic resonance imaging during the previous admission shows a focal, bulging, sac-like lesion (arrow) without a definite peripheral wall in the lateral wall at the mid-LV level. LV: left ventricle.
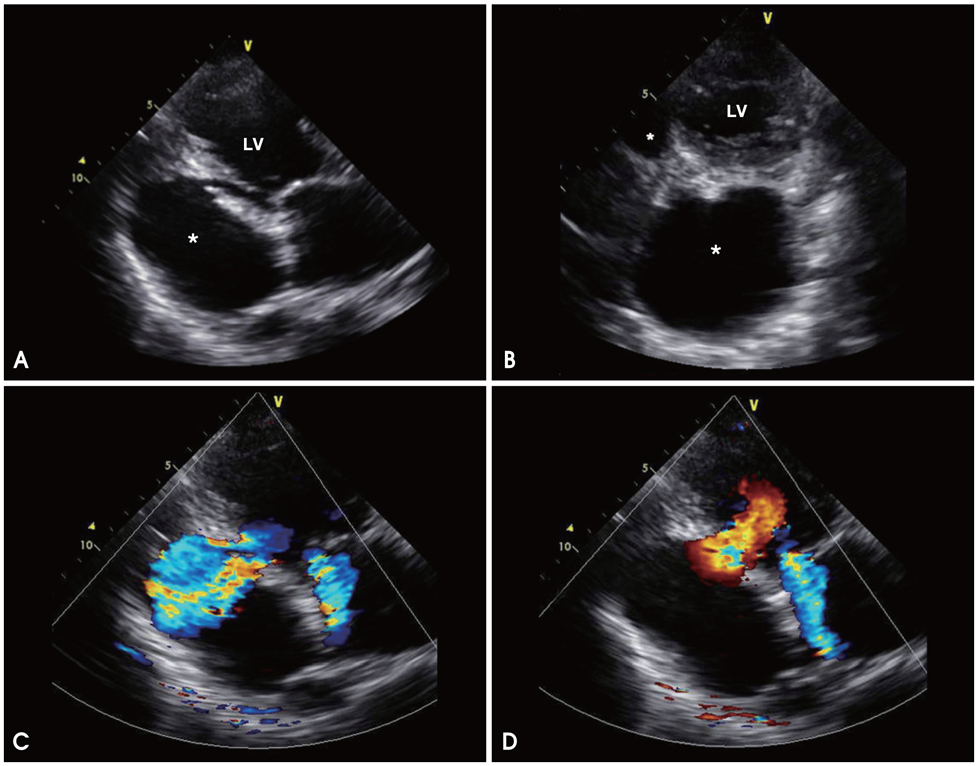
Fig. 4 Transthoracic two-dimensional echocardiography on re-admission shows a large, echo-free space (*) behind the posterior wall, which communicates with the left ventricle through a narrow orifice, and an abrupt interruption of the myocardium at the neck is shown (A and B). The maximal diameter of the cavity is 80×55 mm and that of the orifice is 14×18 mm. A color Doppler study shows the blood fiows across the orifice from the LV to the cavity in systole (C) and from the cavity to the LV in diastole (D). Mild-to-moderate mitral regurgitation is observed in both systole (C) and diastole (D). LV: left ventricle.
Reference
-
1. Frances C, Romero A, Grady D. Left Ventricular Pseudoaneurysm. J Am Coll Cardiol. 1998. 32:557–561.
Article2. Nurozler F, Kutlu T, Küçük G. False aneurysm of the left ventricle following myocardial infarction: an unusual location. Cardiovasc J Afr. 2007. 18:380–382.3. Rittenhouse EA, Sauvage LR, Mansfield PB, Smith JC, Davis CC, Hall DG. False aneurysm of the left ventricle. Report of four cases and review of surgical management. Ann Surg. 1979. 189:409–415.4. Contuzzi R, Gatto L, Patti G, Goffredo C, D'Ambrosio A, Covino E, Chello M, Di Sciascio G. Giant left ventricular pseudoaneurysm complicating an acute myocardial infarction in patient with previous cardiac surgery: a case report. J Cardiovasc Med (Hagerstown). 2009. 10:81–84.
Article5. Turgeman Y, Antonelli D, Rosenfeld T. Intermittent to-and-fro murmur in cardiac pseudoaneurysm: Doppler echocardiographic findings. Int J Cardiol. 1990. 26:376–377.
Article6. MacNeil DJ, Vieweg WV, Oury JH, Folkerth TL, Hagan AD. Pseudomitral regurgitation due to false aneurysm of the left ventricle treated successfully by surgery. Chest. 1974. 66:724–726.
Article7. March KL, Sawada SG, Tarver RD, Kesler KA, Armstrong WF. Current concepts of left ventricular pseudoaneurysm: pathophysiology, therapy, and diagnostic imaging methods. Clin Cardiol. 1989. 12:531–540.
Article8. Brown SL, Gropler RJ, Harris KM. Distinguishing left ventricular aneurysm from pseudoaneurysm. A review of the literature. Chest. 1997. 111:1403–1409.
Article9. Park JR, Kho JS, Im SI, Park JY, Choi BR, Park SJ, Kwak CH, Hwang JY, Jeon KN. A case of left ventricular pseudoaneurysm extending to lateral side of left atrium after myocardial infarction. J Cardiovasc Ultrasound. 2006. 14:29–32.
Article10. Pandian NG. Clinical applications of contrast echocardiography. Eur J Echocardiogr. 2004. 5:Suppl 2. S3–S10.
Article11. Niimura H, Mito T, Matsunaga A, Koga S, Akasu K, Morishige N, Tashiro T, Saku K. Left ventricular pseudoaneurysm following acute myocardial infarction. Intern Med. 2006. 45:1221–1223.
Article12. Konen E, Merchant N, Gutierrez C, Provost Y, Mickleborough L, Paul NS, Butany J. True versus false left ventricular aneurysm: differentiation with MR Imaging--initial experience. Radiology. 2005. 236:65–70.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Left Ventricular Pseudoaneurysm Extending to Lateral Side of Left Atrium after Myocardial Infarction
- A Huge Left Ventricular Pseudoaneurysm after Acute Inferior Myocardial Infarction
- A Case of Asymptomatic Left Ventricular Pseudoaneurysm after Myocardial Infarction
- Incidence of Left Ventricular Thrombus after Acute Myocardial Infarction
- Acute Myocardial Infarction in 14-Year-Old Male of Primary Pulmonary Hypertension with Left Ventricular Hypertrophy : A Case Report
