Predictors of Non-sentinel Lymph Node Metastasis in Breast Cancer
- Affiliations
-
- 1Department of Surgery, Korea Cancer Center Hospital, Seoul, Korea. nohwoo@kcch.re.kr
- 2Department of Pathology, Korea Cancer Center Hospital, Seoul, Korea.
- KMID: 2175007
- DOI: http://doi.org/10.4048/jbc.2007.10.1.95
Abstract
-
PURPOSE: Sentinel lymph node (SLN) biopsy has been shown to be accurate in axillary node staging in early breast cancer. If any SLN is positive, the standard care remains completion axillary node dissection (ALND). However over 50% of the patients with metastatic SLNs do not show other non-SLN metastasis. The purpose of this study was to identify predictors of non-SLN tumor involvement in patients with metastatic SLNs.
METHODS
We reviewed 387 breast cancer patients in whom an SLN biopsy was successfully performed using a subareolar injection of 99mTc-Tin colloid.
RESULTS
Among the reviewed patients, 83 patients showed positive SLNs, and subsequently underwent ALND. In 47 of 83 patients (56.6%), SLNs were the only metastatic nodes. The following factors were assessed for predictors of non- SLN metastasis: age of the patient, size, grade, histologic type, multicentricity of the primary tumor, number of SLNs removed, number of ositive SLNs, number of negative SLNs, size of the SLN metastasis, percentage of SLNs replaced by metastasis, and extracapsular extension (ECE). By multi-variate analysis, the size of SLN metastasis (<2 mm), absence of ECE, and the percent replacement (.10%) were negative predictors of non-SLN metastasis. Among 18 cases in which micrometastasis were found in the SLNs, additional metastasis in non-SLN has been found in 3 cases. This result suggests that micro-metastasis in a SLN is not a sufficient condition for not performing ALND. However, in 9 cases, in which all of three factors (micrometastasis, absence of ECE, no more than 10% replacement of SLNs by tumor cells) were present, additional metastasis had not been found in the non-SLNs.
CONCLUSION
Although further study is needed to verify the result, it would seem that the presence of all three factors (micrometastasis, absence of ECE, no more than 10% replace- ment of SLNs by tumor cells) in combination might be sufficient to safely omit ALND.
Keyword
MeSH Terms
Figure
-

Fig 1 Micrometastasis in SLNs without metastasis in NSLNs. (A) Micrometastasis with less than 10% replacement, without ECE was observed in SLNs (arrow, H&E stain, ×40), (B) No metastasis was found axillary NSLNs (H&E stain, ×10).
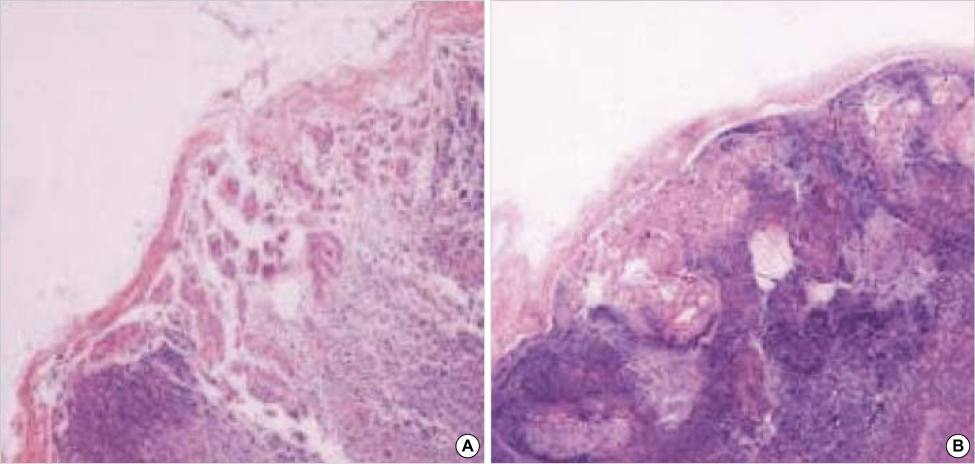
Fig 2 Micrometastasis in SLN with metastasis in NSLN. (A) Micrometastasis with ECE was observed in SLN (H&E stain,×100). (B) Macrometastasis larger than 2 mm was found in one of NSLNs of the same patient (H&E stain, ×40).
Cited by 1 articles
-
A Comparison of Outcomes for the Patients with Pathologically Node-negative Breast Cancer and Who Were Treated Either with Sentinel Lymph Node Biopsy Only or with Conventional Axillary Lymph Node Dissection
Hyun-Ah Kim, Eun-Jeong Jo, Min-Suk Kim, Yang-Hee Kim, Nam-Sun Paik, Nan-Mo Moon, Jong-Inn Lee, Kwang Mo Yang, Woo-Chul Noh
J Breast Cancer. 2009;12(4):265-271. doi: 10.4048/jbc.2009.12.4.265.
Reference
-
1. Fisher ER, Anderson S, Redmond C, Fisher B. Pathologic findings from the National Surgical Adjuvant Breast Project protocol B-06. 10-year pathologic and clinical prognostic discriminants. Cancer. 1993. 71:2507–2514.
Article2. Roses DF, Brooks AD, Harris MN, Shapiro RL, Mitnick J. Complications of level I and II axillary dissection in the treatment of carcinoma of the breast. Ann Surg. 1999. 230:194–201.
Article3. Hack TF, Cohen L, Katz J, Robson LS, Goss P. Physical and psychological morbidity after axillary lymph node dissection for breast cancer. J Clin Oncol. 1999. 17:143–149.
Article4. Velanovich V, Szymanski W. Quality of life of breast cancer patients with lymphedema. Am J Surg. 1999. 177:184–187.
Article5. Miltenburg DM, Miller C, Karamlou TB, Brunicardi FC. Metaanalysis of sentinel lymph node biopsy in breast cancer. J Surg Res. 1999. 84:138–142.
Article6. Morrow M. Is axillary dissection necessary after positive sentinel node biopsy? Yes! Ann Surg Oncol. 2001. 8:S74–S76.7. Krag D, Weaver D, Ashikaga T, Moffat F, Klimberg VS, Shriver C, et al. The sentinel node in breast cancer- a multicenter validation study. N Engl J Med. 1998. 339:941–946.
Article8. Bass SS, Cox CE, Ku NN, Berman C, Reintgen DS. The role of sentinel lymph node biopsy in breast cancer. J Am Coll Surg. 1999. 189:183–194.9. Kim KS, Kim YH, Paik NS, Kim MS, Choi CW, Moon NM, et al. Utility of breast sentinel lymph node biopsy using the day-before or the same-day subareolar injection of 99mTc-Tin colloid. J Breast Cancer. 2006. 9:121–126.
Article10. Lee HD, Choi JW, Kim DY, Park BW, Lee IK, Song HJ, et al. Clinical experience for sentinel lymphadenectomy alone in early breast cancer. J Korean Breast Cancer Soc. 2003. 6:263–270.
Article11. Lee IK, Lee SA, Jeong J, Park BW, Jung WH, Hong SW, et al. Predicting the status of the nonsentinel lymph nodes in early breast cancer patients with positive sentinel lymph nodes. J Korean Breast Cancer Soc. 2004. 7:268–274.
Article12. van Iterson V, Leidenius M, Krogerus L, von Smitten K. Predictive factors for the status of non-sentinel nodes in breast cancer patients with tumor positive sentinel nodes. Breast Cancer Res Treat. 2003. 82:39–45.
Article13. Chu KU, Turner RR, Hansen NM, Brennan MB, Bilchik A, Giuliano AE. Do all patients with sentinel node metastasis from breast carcinoma need complete axillary node dissection? Ann Surg. 1999. 229:536–541.
Article14. Changsri C, Prakash S, Sandweiss L, Bose S. Prediction of additional axillary metastasis of breast cancer following sentinel lymph node surgery. Breast J. 2004. 10:392–397.
Article15. Joseph KA, EI-Tamer M, Komenaka I, Troxel A, Ditkoff BA, Schnabel F. Predictors of nonsentinel node metastasis in patients with breast cancer after sentinel node metastasis. Arch Surg. 2004. 139:648–651.
Article16. Stitzenberg KB, Meyer AA, Stern SL, Cance WG, Calvo BF, Klauber-DeMore N, et al. Extracapsular extension of the sentinel lymph node metastasis: a predictor of nonsentinel node tumor burden. Ann Surg. 2003. 237:607–613.
Article17. Travagli JP, Atallah D, Mathieu MC, Rochard F, Camatte S, Lumbroso J, et al. Sentinel lymphadenectomy without systematic axillary dissection in breast cancer patients: predictors of non-sentinel lymph node metastasis. Eur J Surg Oncol. 2003. 29:403–406.
Article18. Saidi RF, Dudrick PS, Remine SG, Mittal VK. Nonsentinel lymph node status after positive sentinel lymph node biopsy in early breast cancer. Am Surg. 2004. 70:101–105.19. Wong SL, Edwards MJ, Chao C, Tuttle TM, Noyes RD, Woo C, et al. Predicting the status of the nonsentinel axillary nodes: a multicenter study. Arch Surg. 2001. 136:563–568.
Article20. Rahusen FD, Torrenga H, van Diest PJ, Pijpers R, van der Wall E, Licht J, et al. Predictive factors for metastatic involvement of nonsentinel nodes in patients with breast cancer. Arch Surg. 2001. 136:1059–1063.
Article21. Goyal A, Douglas-Jones A, Newcombe RG, Mansel RE. ALMANAC Trialists Group. Predictors of non-sentinel lymph node metastasis in breast cancer patients. Eur J Cancer. 2004. 40:1731–1737.
Article22. Liang WC, Sickle-Santanello BJ, Nims TA. Is a completion axillary dissection indicated for micrometastases in the sentinel lymph node? Am J Surg. 2001. 182:365–368.
Article23. Gipponi M, Canavese G, Lionetto R, Catturich A, Vecchio C, Sapino A, et al. The role of axillary lymph node dissection in breast cancer patients with sentinel lymph node micrometastases. Eur J Surg Oncol. 2006. 32:143–147.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sentinel Lymph Node Biopsy in Breast Cancer: A Clinical Review and Update
- The Number of Removed Lymph Nodes for an Acceptable False Negative Rate in Sentinel Lymph Node Biopsy for Breast Cancer
- Validation and Controversy of Sentinel Node Biopsy for Breast Cancer
- Intramammary sentinel lymph node with capsular extravasation in breast cancer
- Sentinel Lymph Node Imaging in Breast Cancer
