A Case of Erdheim-Chester Disease with Asymptomatic Renal Involvement
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. gabriel9@snu.ac.kr
- 2Department of Pathology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Orthopedic Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
Abstract
- Erdheim-Chester disease is a rare non-Langerhans-cell histiocytosis involving bones and multiple organs. Its clinical course can vary, from an asymptomatic state to a fatal disease, with renal involvement being a common cause of death. A 41-year-old man presented with a 10-month history of bilateral lower limb pain. Left perirenal soft-tissue infiltration had been found incidentally two years earlier. No progression of the lesion or deterioration of renal function was observed for a period of two years. At admission, plain radiography and magnetic resonance imaging of the patient's lower limbs showed patchy osteosclerosis. Biopsy of the tibia revealed histiocytic infiltration, which was found to be positive for CD68 and negative for CD1a. This report describes an unusual case of Erdheim-Chester disease involving a stationary course of disease with no specific treatment for a long period of time.
MeSH Terms
Figure
-
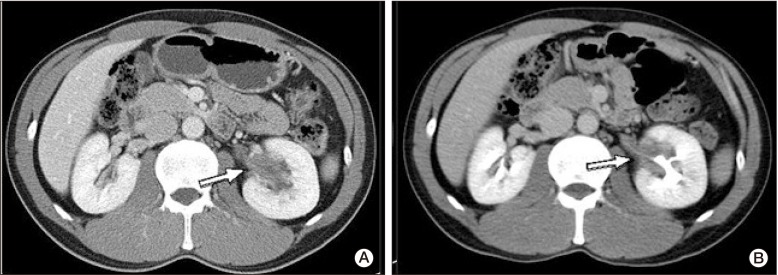
Fig. 1 Computed tomography (CT) scan of the patient's abdomen in 2008 showed tissue infiltration with low attenuation surrounding the left renal sinus and the proximal ureter (A). No significant change was observed on CT scan in 2010 (B).

Fig. 2 Simple radiography of the left knee showed heterogeneous patchy medullary sclerosis, coarse trabeculae, and osteopenia of the covered femur and tibia (A). Magnetic resonance imaging of the knee showed diffuse sclerotic changes combined with intramedullary low signal intensity on a T1-weighted image (B) and mixed low- and high-signal nodular lesions on a T2-weighted image (C). Involvement of mainly the meta- and diaphysis, with relative epiphyseal sparing, was observed.
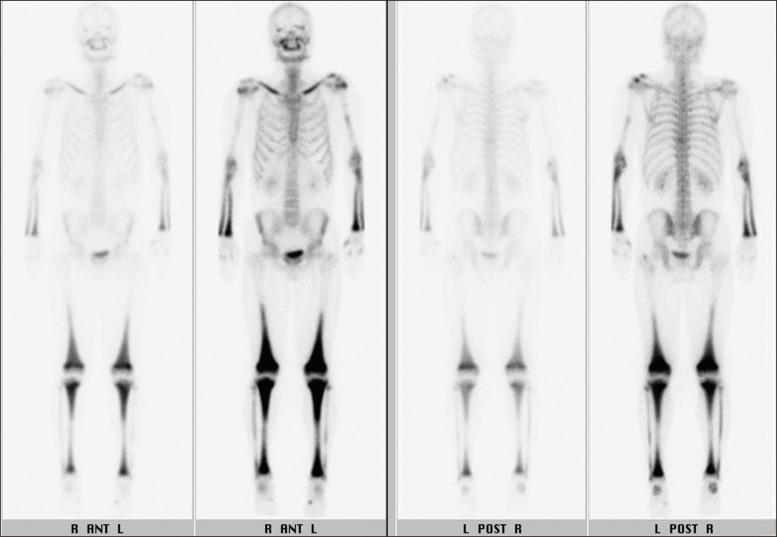
Fig. 3 Whole-body bone scintigraphy revealed diffuse increased uptake in the bilateral clavicles, radii, ulnae, distal femora, tibiae, and fibulae.
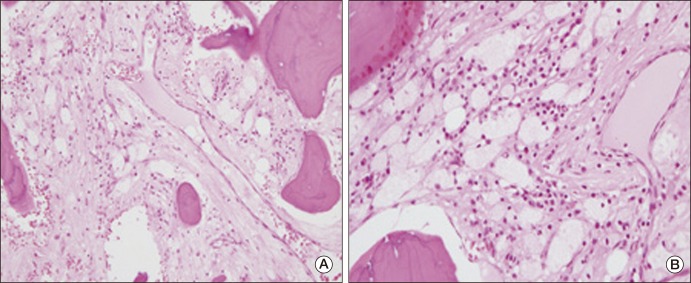
Fig. 4 Results of hematoxylin and eosin staining showed sclerotic bony trabeculae containing lipid-laden histiocytes and small histiocytes with oval nuclei and pink cytoplasm. A small number of infiltrating inflammatory cells were observed; however, eosinophils were rare (A, ×200; B, ×400).
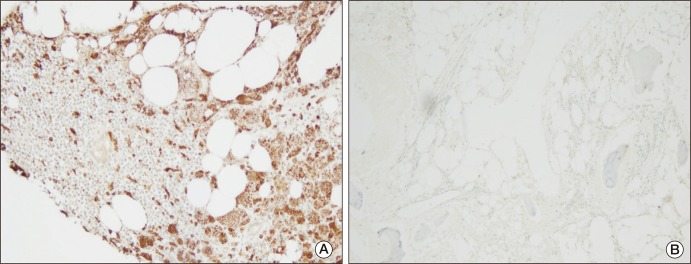
Fig. 5 Lipid-laden histiocytes were positive for CD68 (A, CD68 immunostain, ×100). Histiocytes were negative for CD1a (B, CD1a immunostain, ×200).
Reference
-
1. Chester W. Über lipoidgranulomatose. Virchows Arch Pathol Anat Physiol. 1930; 279:561–602.
Article2. Park YK, Ryu KN, Huh B, Kim JD. Erdheim-Chester disease: a case report. J Korean Med Sci. 1999; 14:323–326. PMID: 10402177.
Article3. Veyssier-Belot C, Cacoub P, Caparros-Lefebvre D, Wechsler J, Brun B, Remy M, et al. Erdheim-Chester disease. Clinical and radiologic characteristics of 59 cases. Medicine (Baltimore). 1996; 75:157–169. PMID: 8965684.
Article4. Zelger B, Cerio R, Orchard G, Wilson-Jones E. Juvenile and adult xanthogranuloma. A histological and immunohistochemical comparison. Am J Surg Pathol. 1994; 18:126–135. PMID: 8291651.5. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 9-2000 A 41-year-old man with multiple bony lesions and adjacent soft-tissue masses. N Engl J Med. 2000; 342:875–883. PMID: 10727593.6. Weitzman S, Jaffe R. Uncommon histiocytic disorders: the non-Langerhans cell histiocytoses. Pediatr Blood Cancer. 2005; 45:256–264. PMID: 15547923.
Article7. Mossetti G, Rendina D, Numis FG, Somma P, Postiglione L, Nunziata V. Biochemical markers of bone turnover, serum levels of interleukin-6/interleukin-6 soluble receptor and bisphosphonate treatment in Erdheim-Chester disease. Clin Exp Rheumatol. 2003; 21:232–236. PMID: 12747282.8. Boissel N, Wechsler B, Leblond V. Treatment of refractory Erdheim-Chester disease with double autologous hematopoietic stem-cell transplantation. Ann Intern Med. 2001; 135:844–845. PMID: 11694122.
Article9. Haroche J, Amoura Z, Trad SG, Wechsler B, Cluzel P, Grenier PA, et al. Variability in the efficacy of interferon-alpha in Erdheim-Chester disease by patient and site of involvement: results in eight patients. Arthritis Rheum. 2006; 54:3330–3336. PMID: 17009306.10. Braiteh F, Boxrud C, Esmaeli B, Kurzrock R. Successful treatment of Erdheim-Chester disease, a non-Langerhans-cell histiocytosis, with interferon-alpha. Blood. 2005; 106:2992–2994. PMID: 16020507.11. Suzuki HI, Hosoya N, Miyagawa K, Ota S, Nakashima H, Makita N, et al. Erdheim-Chester disease: multisystem involvement and management with interferon-alpha. Leuk Res. 2010; 34:e21–e24. PMID: 19679354.12. Sanchez JE, Mora C, Macia M, Navarro JF. Erdheim-Chester disease as cause of end-stage renal failure: a case report and review of the literature. Int Urol Nephrol. 2010; 42:1107–1112. PMID: 20232144.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Commentary on "A Case of Erdheim-Chester Disease with Asymptomatic Renal Involvement"
- Reply to Commentary on "A Case of Erdheim-Chester Disease with Asymptomatic Renal Involvement"
- Erdheim-Chester Disease with Perirenal Masses Containing Macroscopic Fat Tissue
- Erdheim–Chester Disease Involving the Biliary System and Mimicking Immunoglobulin G4-Related Disease: A Case Report
- A Case of Erdheim-Chester Disease with Bilateral Hydronephrosis
