The effects of the end-to-side inverted mattress pancreaticojejunostomy on postoperative pancreatic fistula: a single surgeon's experience
- Affiliations
-
- 1Department of Surgery, Kyungpook National University Medical Center, Daegu, Korea. ksg@knu.ac.kr
- 2Department of Surgery, Kyungpook National University School of Medicine, Daegu, Korea.
- KMID: 2166972
- DOI: http://doi.org/10.4174/astr.2015.89.2.61
Abstract
- PURPOSE
Various pancreaticojejunostomy (PJ) techniques have been devised to minimize the rate of postoperative pancreatic fistula (POPF) after pancreatoduodenectomy (PD). This study describes a modification of the mattress suture PJ technique, which we call "inverted mattress PJ (IM)". The results of an IM group and a historical consecutive control group were compared to determine how the IM technique affected POPF.
METHODS
From 2003 to 2010, 186 consecutive patients underwent PD. A former group of 52 consecutive patients who underwent conventional duct-to-mucosa PJ (DM) was used as a historical control group. The IM technique was utilized for the IM group (134 patients). The clinicopathological features and surgical outcomes of the 2 groups were compared, with a particular focus on postoperative POPFs.
RESULTS
The average surgery duration was shorter in the IM group (580.3 minutes vs. 471 minutes, P < 0.001). Grades B and C POPFs occurred less frequently in the IM group, but the difference was not statistically significant (17.3% vs. 9.7%, P = 0.200). However, no grade C POPF occurred in the IM group compared with 5.8% of grade C POPFs (3/52) in the DM group (P = 0.020). Three patients died (1 in the DM group and 2 in the IM group). The causes of death were arrhythmia in 2 cases and Candida sepsis in 1 case. POPF was not causally related to the 3 deaths.
CONCLUSION
IM end-to-side PJ shortened operation time and increased safety with no incidence of grade C POPF.
Keyword
MeSH Terms
Figure
-
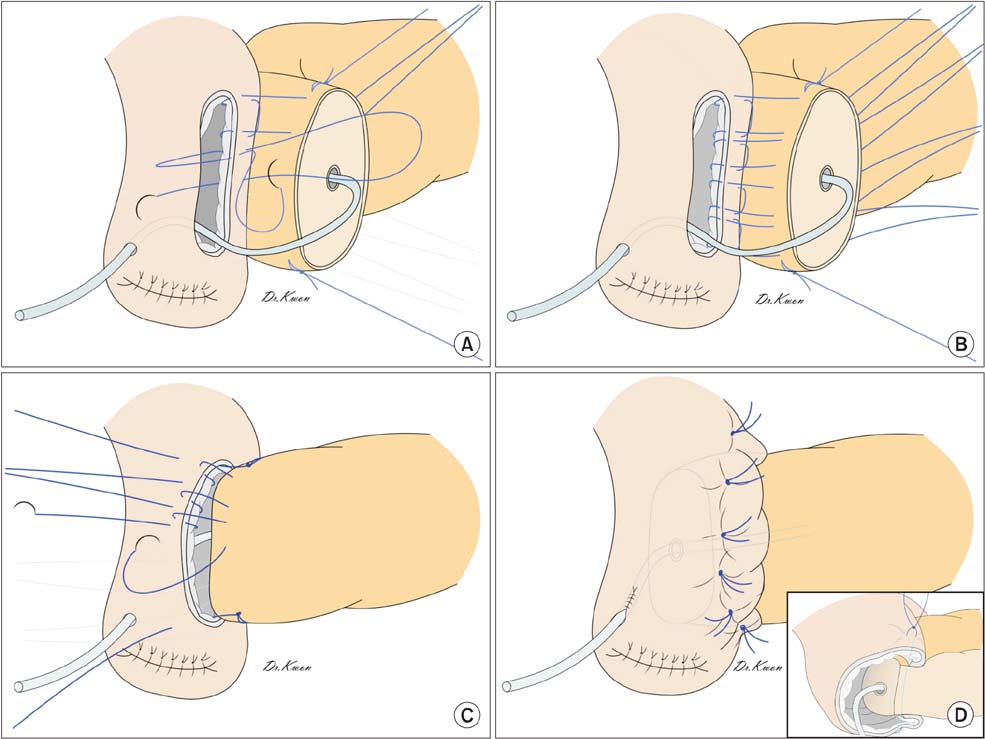
Fig. 1 (A) Three to four U-shaped mattress sutures (4-0 Prolene, Ethicon Inc., Somerville, NJ, USA) were placed starting at the serosa of the posterior jejunal wall. The inverted seromuscular stitches were made going in-out. (B) These sutures penetrated the pancreatic remnant in a straight manner. (C) After penetrating the pancreatic parenchyma with a needle, the seromuscular layer of the anterior jejunal wall was inverted with the sutures going out-in, followed by a full thickness stitch of the anterior jejunal wall going in-out. (D) The U-shaped sutures were pulled with adequate tension and tied at the anterior wall and both corners of the jejunum. The cross-sectional view of the pancreaticojejunostomy shows the pancreatic remnant fully invaginated into the lumen of the jejunum. Tying all stitches encloses the jejunal opening around the pancreas remnant.
Cited by 1 articles
-
Unfavorable effect of high postoperative fluid balance on outcome of pancreaticoduodenectomy
Hyun-Jeong Jeon, Hyung-Jun Kwon, Yoon-Jin Hwang, Sang-Geol Kim
Ann Surg Treat Res. 2022;102(3):139-146. doi: 10.4174/astr.2022.102.3.139.
Reference
-
1. Crist DW, Sitzmann JV, Cameron JL. Improved hospital morbidity, mortality, and survival after the Whipple procedure. Ann Surg. 1987; 206:358–365.2. Fong Y, Gonen M, Rubin D, Radzyner M, Brennan MF. Long-term survival is superior after resection for cancer in high-volume centers. Ann Surg. 2005; 242:540–544.3. Ho V, Heslin MJ. Effect of hospital volume and experience on in-hospital mortality for pancreaticoduodenectomy. Ann Surg. 2003; 237:509–514.4. Schmidt CM, Powell ES, Yiannoutsos CT, Howard TJ, Wiebke EA, Wiesenauer CA, et al. Pancreaticoduodenectomy: a 20-year experience in 516 patients. Arch Surg. 2004; 139:718–725.5. Ho CK, Kleeff J, Friess H, Buchler MW. Complications of pancreatic surgery. HPB (Oxford). 2005; 7:99–108.6. Lin JW, Cameron JL, Yeo CJ, Riall TS, Lillemoe KD. Risk factors and outcomes in postpancreaticoduodenectomy ancreaticocutaneous fistula. J Gastrointest Surg. 2004; 8:951–959.7. Bartoli FG, Arnone GB, Ravera G, Bachi V. Pancreatic fistula and relative mortality in malignant disease after pancreaticoduodenectomy. Review and statistical meta-analysis regarding 15 years of literature. Anticancer Res. 1991; 11:1831–1848.8. Tsiotos GG, Farnell MB, Sarr MG. Are the results of pancreatectomy for pancreatic cancer improving? World J Surg. 1999; 23:913–919.9. Poon RT, Lo SH, Fong D, Fan ST, Wong J. Prevention of pancreatic anastomotic leakage after pancreaticoduodenectomy. Am J Surg. 2002; 183:42–52.10. Bassi C, Falconi M, Salvia R, Mascetta G, Molinari E, Pederzoli P. Management of complications after pancreaticoduodenectomy in a high volume centre: results on 150 consecutive patients. Dig Surg. 2001; 18:453–457.11. Yeo CJ, Cameron JL, Sohn TA, Lillemoe KD, Pitt HA, Talamini MA, et al. Six hundred fifty consecutive pancreaticoduodenectomies in the 1990s: pathology, complications, and outcomes. Ann Surg. 1997; 226:248–257.12. Balcom JH 4th, Rattner DW, Warshaw AL, Chang Y, Fernandez-del Castillo C. Ten-year experience with 733 pancreatic resections: changing indications, older patients, and decreasing length of hospitalization. Arch Surg. 2001; 136:391–398.13. Tewari M, Hazrah P, Kumar V, Shukla HS. Options of restorative pancreaticoenteric anastomosis following pancreaticoduodenectomy: a review. Surg Oncol. 2010; 19:17–26.14. Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005; 138:8–13.15. Langrehr JM, Bahra M, Jacob D, Glanemann M, Neuhaus P. Prospective randomized comparison between a new mattress technique and Cattell (duct-to-mucosa) pancreaticojejunostomy for pancreatic resection. World J Surg. 2005; 29:1111–1119.16. Yeh TS, Jan YY, Jeng LB, Hwang TL, Wang CS, Chen SC, et al. Pancreaticojejunal anastomotic leak after pancreaticoduodenectomy: multivariate analysis of perioperative risk factors. J Surg Res. 1997; 67:119–125.17. Yang YM, Tian XD, Zhuang Y, Wang WM, Wan YL, Huang YT. Risk factors of pancreatic leakage after pancreaticoduodenectomy. World J Gastroenterol. 2005; 11:2456–2461.18. Strasberg SM, McNevin MS. Results of a technique of pancreaticojejunostomy that optimizes blood supply to the pancreas. J Am Coll Surg. 1998; 187:591–596.19. Kleespies A, Rentsch M, Seeliger H, Albertsmeier M, Jauch KW, Bruns CJ. Blumgart anastomosis for pancreaticojejunostomy minimizes severe complications after pancreatic head resection. Br J Surg. 2009; 96:741–750.20. Grobmyer SR, Kooby D, Blumgart LH, Hochwald SN. Novel pancreaticojejunostomy with a low rate of anastomotic failure-related complications. J Am Coll Surg. 2010; 210:54–59.21. Pratt WB, Maithel SK, Vanounou T, Huang ZS, Callery MP, Vollmer CM Jr. Clinical and economic validation of the International Study Group of Pancreatic Fistula (ISGPF) classification scheme. Ann Surg. 2007; 245:443–451.22. Fuks D, Piessen G, Huet E, Tavernier M, Zerbib P, Michot F, et al. Life-threatening postoperative pancreatic fistula (grade C) after pancreaticoduodenectomy: incidence, prognosis, and risk factors. Am J Surg. 2009; 197:702–709.23. Reid-Lombardo KM, Farnell MB, Crippa S, Barnett M, Maupin G, Bassi C, et al. Pancreatic anastomotic leakage after pancreaticoduodenectomy in 1,507 patients: a report from the Pancreatic Anastomotic Leak Study Group. J Gastrointest Surg. 2007; 11:1451–1458.24. Liang TB, Bai XL, Zheng SS. Pancreatic fistula after pancreaticoduodenectomy: diagnosed according to International Study Group Pancreatic Fistula (ISGPF) definition. Pancreatology. 2007; 7:325–331.25. Kollmar O, Moussavian MR, Bolli M, Richter S, Schilling MK. Pancreatojejunal leakage after pancreas head resection: anatomic and surgeon-related factors. J Gastrointest Surg. 2007; 11:1699–1703.26. Pratt WB, Callery MP, Vollmer CM Jr. Risk prediction for development of pancreatic fistula using the ISGPF classification scheme. World J Surg. 2008; 32:419–428.27. Sato N, Yamaguchi K, Chijiiwa K, Tanaka M. Risk analysis of pancreatic fistula after pancreatic head resection. Arch Surg. 1998; 133:1094–1098.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Utilization of end to side inverted mattress pancreaticojejunostomy for Duval procedure: A case report
- The Complication Rate according to the Method of Pancreaticojejunostomy after Pancreaticoduodenectomy
- Effect of end-to-side inverted mattress pancreaticojejunostomy following central pancreatectomy on the prevention of pancreatic fistula
- Pancreatic Fistula after Pancreaticoduodenectomy: A Comparison between the Two Pancreaticojejunostomy Methods for Approximating the Pancreatic Parenchyma to the Jejunal Seromuscular Layer: Interrupted Vs. Continuous Stitches
- Current Definition of and Controversial Issues Regarding Postoperative Pancreatic Fistulas
