Diagnostic Decision Points of Specific IgE Concentrations in Korean Children With Egg and Cow's Milk Allergies
- Affiliations
-
- 1Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. kmaped@skku.edu.
- 2Environmental Health Center for Atopic Diseases, Samsung Medical Center, Seoul, Korea.
- 3Department of Pediatrics, Medical Research Institute of Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea.
- 4Department of Biostatistics, Samsung Biomedical Research Institute, Seoul, Korea.
- KMID: 2166680
- DOI: http://doi.org/10.4168/aair.2015.7.4.332
Abstract
- PURPOSE
The purpose of this study was to evaluate the utility of specific IgE (sIgE) concentrations for the diagnosis of immediate-type egg and cow's milk (CM) allergies in Korean children and to determine the optimal cutoff levels.
METHODS
In this prospective study, children > or =12 months of age with suspected egg or CM allergy were enrolled. Food allergy was diagnosed by an open oral food challenge (OFC) or through the presence of a convincing history after ingestion of egg or CM. The cutoff levels of sIgE for egg white (EW) and CM were determined by analyzing the receiver operating characteristic curves.
RESULTS
Out of 273 children, 52 (19.0%) were confirmed to have egg allergy. CM allergy was found in 52 (23.1%) of 225 children. The EW-sIgE concentration indicating a positive predictive value (PPV) of >90% was 28.1 kU/L in children <24 months of age and 22.9 kU/L in those > or =24 months of age. For CM-sIgE, the concentration of 31.4 kU/L in children <24 months of age and 10.1 kU/L in those > or =24 months of age indicated a >90% PPV. EW-sIgE levels of 3.45 kU/L presented a negative predictive value (NPV) of 93.6% in children <24 months of age, while 1.80 kU/L in those > or =24 months of age presented a NPV of 99.2%. The CM-sIgE levels of 0.59 kU/L in children <24 months of age and 0.94 kU/L in those > or =24 months of age showed NPVs of 100% and 96.9%.
CONCLUSIONS
Our results indicate that different diagnostic decision points (DDPs) of sIgE levels should be used for the diagnosis of egg or CM allergy in Korean children. The data also suggest that DDPs with high PPV and high NPV are useful for determining whether OFC is required in children with suspected egg or CM allergy.
Keyword
MeSH Terms
Figure
-

Fig. 1 Flowchart of study population.

Fig. 2 Comparison of specific IgE levels between positive and negative oral food challenge (OFC) groups. (A) All children for hen's egg challenge; (B) those <24 months of age for hen's egg challenge; (C) those ≥24 months of age for hens' egg challenge; (D) all children for cow's milk challenge; (E) those <24 months of age for cow's milk challenge; (F) those ≥24 months of age for cow's milk challenge. EW, egg white; CM, cow's milk. Each box plot indicates an interquartile range (IQR) with median, upper, and lower whiskers; upper and lower boundaries (3rd quartile/1st quartile ±1.5 IQR). The blue and red boxes represent patients showing positive and negative OFC results.
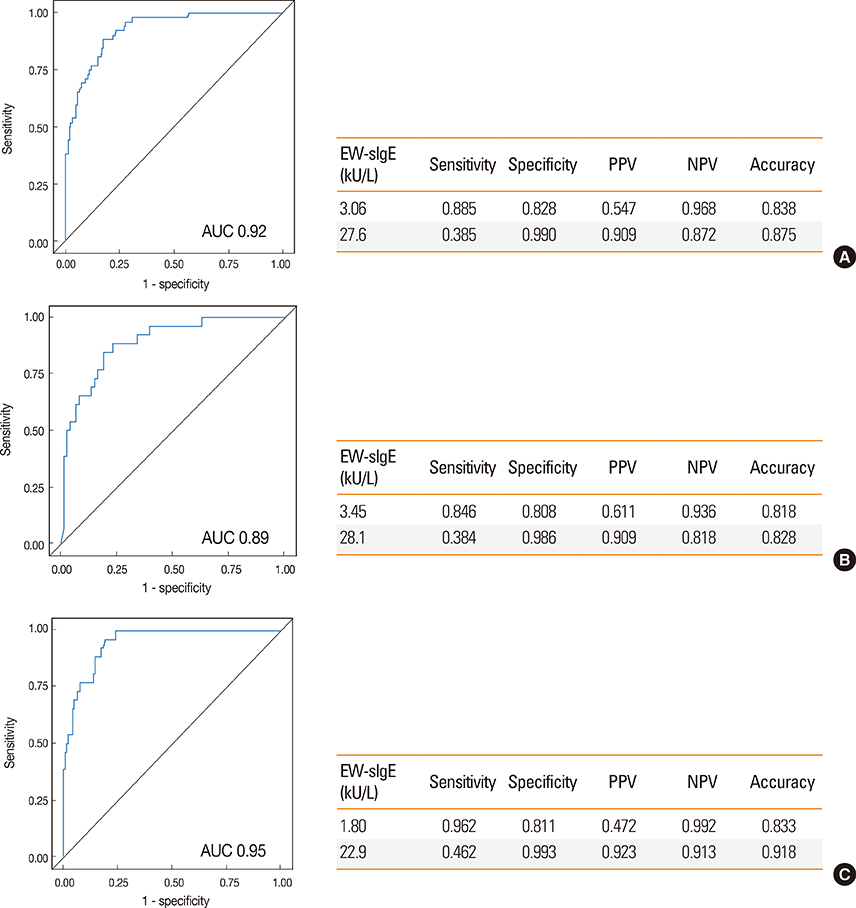
Fig. 3 Performance characteristics of optimal cutoff values of egg white specific IgE established by ROC analysis. (A) All children; (B) those <24 months of age; (C) those ≥24 months of age.
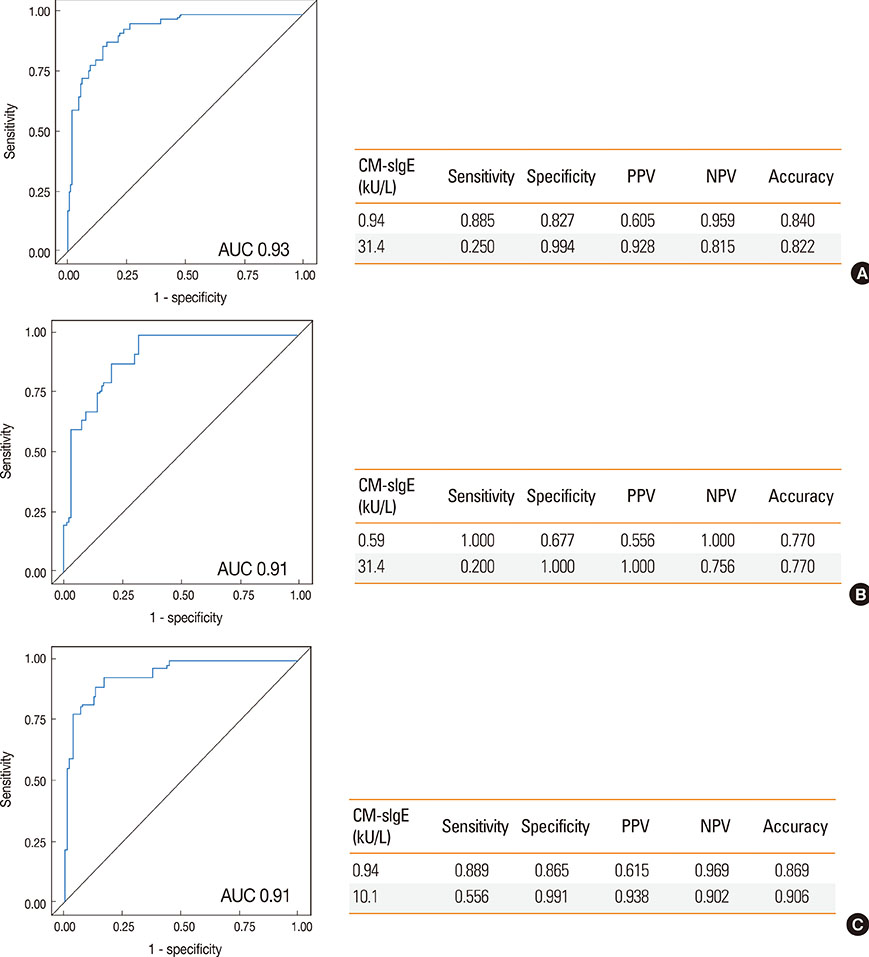
Fig. 4 Performance characteristics of optimal cutoff values of cow's milk specific IgE established by ROC analysis. (A) All children; (B) those <24 months of age; (C) those ≥24 months of age.
Cited by 5 articles
-
Infantile Anaphylaxis in Korea: a Multicenter Retrospective Case Study
You Hoon Jeon, Sooyoung Lee, Kangmo Ahn, So-Yeon Lee, Kyung Won Kim, Hyun Hee Kim, Jeong Hee Kim, Hye Yung Yum, Woo Kyung Kim, Yong Mean Park, Tae Won Song, Jihyun Kim, Yong Ju Lee, Gwang Cheon Jang, Kyunguk Jeong, Yoon Hee Kim, Taek Ki Min, Bok Yang Pyun,
J Korean Med Sci. 2019;34(13):. doi: 10.3346/jkms.2019.34.e106.Food allergy in children: focus on IgE-mediated food allergy
Sooyoung Lee
J Korean Med Assoc. 2017;60(3):242-248. doi: 10.5124/jkma.2017.60.3.242.Sensitization in children with atopic dermatitis: a single center study
Ari Song, Ji Young Lee, Hea-kyoung Yang, Minji Kim, Kangmo Ahn, Sang-il Lee, Jihyun Kim
Allergy Asthma Respir Dis. 2016;4(4):290-295. doi: 10.4168/aard.2016.4.4.290.The past, present, and future of the research on food allergy in Korean children
Kangmo Ahn
Allergy Asthma Respir Dis. 2018;6(Suppl 1):S44-S51. doi: 10.4168/aard.2018.6.S1.S44.Oral food challenges: result of a 16-year experience at a major teaching hospital in Thailand
Witchaya Srisuwatchari, Pakit Vichyanond
Asia Pac Allergy. 2018;8(2):. doi: 10.5415/apallergy.2018.8.e21.
Reference
-
1. Lee AJ, Thalayasingam M, Lee BW. Food allergy in Asia: how does it compare? Asia Pac Allergy. 2013; 3:3–14.2. Berni Canani R, Ruotolo S, Discepolo V, Troncone R. The diagnosis of food allergy in children. Curr Opin Pediatr. 2008; 20:584–589.3. Ramesh S. Food allergy overview in children. Clin Rev Allergy Immunol. 2008; 34:217–230.4. Kim J, Chang E, Han Y, Ahn K, Lee SI. The incidence and risk factors of immediate type food allergy during the first year of life in Korean infants: a birth cohort study. Pediatr Allergy Immunol. 2011; 22:715–719.5. Park M, Kim D, Ahn K, Kim J, Han Y. Prevalence of immediate-type food allergy in early childhood in Seoul. Allergy Asthma Immunol Res. 2014; 6:131–136.6. Celik-Bilgili S, Mehl A, Verstege A, Staden U, Nocon M, Beyer K, et al. The predictive value of specific immunoglobulin E levels in serum for the outcome of oral food challenges. Clin Exp Allergy. 2005; 35:268–273.7. NIAID-Sponsored Expert Panel. Boyce JA, Assa'ad A, Burks AW, Jones SM, Sampson HA, et al. Guidelines for the diagnosis and management of food allergy in the United States: report of the NIAID-sponsored expert panel. J Allergy Clin Immunol. 2010; 126:S1–S58.8. Gupta RS, Dyer AA, Jain N, Greenhawt MJ. Childhood food allergies: current diagnosis, treatment, and management strategies. Mayo Clin Proc. 2013; 88:512–526.9. Sampson HA. Food allergy--accurately identifying clinical reactivity. Allergy. 2005; 60:Suppl 79. 19–24.10. Sampson HA, Ho DG. Relationship between food-specific IgE concentrations and the risk of positive food challenges in children and adolescents. J Allergy Clin Immunol. 1997; 100:444–451.11. Sampson HA. Update on food allergy. J Allergy Clin Immunol. 2004; 113:805–819.12. Boyano Martínez T, García-Ara C, Díaz-Pena JM, Muñoz FM, García Sánchez G, Esteban MM. Validity of specific IgE antibodies in children with egg allergy. Clin Exp Allergy. 2001; 31:1464–1469.13. Sicherer SH, Sampson HA. Food allergy. J Allergy Clin Immunol. 2010; 125:S116–S125.14. Rolinck-Werninghaus C, Niggemann B, Grabenhenrich L, Wahn U, Beyer K. Outcome of oral food challenges in children in relation to symptom-eliciting allergen dose and allergen-specific IgE. Allergy. 2012; 67:951–957.15. Longo G, Berti I, Burks AW, Krauss B, Barbi E. IgE-mediated food allergy in children. Lancet. 2013; 382:1656–1664.16. Komata T, Söderström L, Borres MP, Tachimoto H, Ebisawa M. The predictive relationship of food-specific serum IgE concentrations to challenge outcomes for egg and milk varies by patient age. J Allergy Clin Immunol. 2007; 119:1272–1274.17. Min TK, Jeon YH, Yang HJ, Pyun BY. The clinical usefulness of IgE antibodies against egg white and its components in Korean children. Allergy Asthma Immunol Res. 2013; 5:138–142.18. Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol Suppl (Stockh). 1980; 60:44–47.19. Song TW, Kim KW, Kim WK, Kim JH, Kim HH, Park YM, et al. Guidelines for the oral food challenges in children. Pediatr Allergy Respir Dis. 2012; 22:4–20.20. Yum HY, Yang HJ, Kim KW, Song TW, Kim WK, Kim JH, et al. Oral food challenges in children. Korean J Pediatr. 2011; 54:6–10.21. Nowak-Wegrzyn A, Assa'ad AH, Bahna SL, Bock SA, Sicherer SH, Teuber SS, et al. Work Group report: oral food challenge testing. J Allergy Clin Immunol. 2009; 123:S365–S383.22. Bindslev-Jensen C, Ballmer-Weber BK, Bengtsson U, Blanco C, Ebner C, Hourihane J, et al. Standardization of food challenges in patients with immediate reactions to foods--position paper from the European Academy of Allergology and Clinical Immunology. Allergy. 2004; 59:690–697.23. Cianferoni A, Spergel JM. Food allergy: review, classification and diagnosis. Allergol Int. 2009; 58:457–466.24. Roehr CC, Reibel S, Ziegert M, Sommerfeld C, Wahn U, Niggemann B. Atopy patch tests, together with determination of specific IgE levels, reduce the need for oral food challenges in children with atopic dermatitis. J Allergy Clin Immunol. 2001; 107:548–553.25. Sampson HA. Utility of food-specific IgE concentrations in predicting symptomatic food allergy. J Allergy Clin Immunol. 2001; 107:891–896.26. Osterballe M, Bindslev-Jensen C. Threshold levels in food challenge and specific IgE in patients with egg allergy: is there a relationship? J Allergy Clin Immunol. 2003; 112:196–201.27. Burks AW, Jones SM, Boyce JA, Sicherer SH, Wood RA, Assa'ad A, et al. NIAID-sponsored 2010 guidelines for managing food allergy: applications in the pediatric population. Pediatrics. 2011; 128:955–965.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Serum Specific IgE to Egg White, Cow's Milk, Soybean in the Children with Atopic Dermatitis
- The effect of baked egg and milk consumption on IgE-mediated egg and milk allergies in young children
- Analysis of cow's milk specific IgE positive patients in newborns
- Patch Test and Specific IgE Level with Food Antigens in Atopic Dermatitis Patients
- Food Allergy
