Clin Endosc.
2016 Jan;49(1):30-36. 10.5946/ce.2016.49.1.30.
Novel Endoscopic Management of Obesity
- Affiliations
-
- 1Department of Surgery, Polyclinique Lyon-Nord, Rillieux-la-Pape, France. jerome.dargent@polyclinique-rillieux.fr
- KMID: 2166546
- DOI: http://doi.org/10.5946/ce.2016.49.1.30
Abstract
- Endoscopic procedures have been well-documented in the obesity field, but have not yet reached a sufficient level of evidence as stand-alone methods for treating obesity. It is unclear if they should take over. Although expanding, the array of bariatric surgical techniques does not fully meet the current needs, and there are not enough resources for increasing surgery. Surgery is avoided by a majority of patients, so that less aggressive procedures are necessary. For the time being, relevant endoscopic methods include intra-gastric balloons, gastric partitioning (Endo-plication), and the metabolic field (Endo-barrier). Surgical novelties and basic research are also important contributors owing to their potential combination with endoscopy. Conditions have been listed for implementation of bariatric endoscopy, because innovation is risky, expensive, and faces ethical challenges. A scientific background is being built (e.g., hormonal studies). Some techniques require additional study, while others are not ready but should be priorities. Steps and goals include the search for conceptual similarities and the respect of an ethical frame. Minimally invasive bariatric techniques are not ready for prime time, but they are already being successful as re-do procedures. A time-frame for step-strategies can be defined, and more investments from the industry are mandatory.
Figure
-
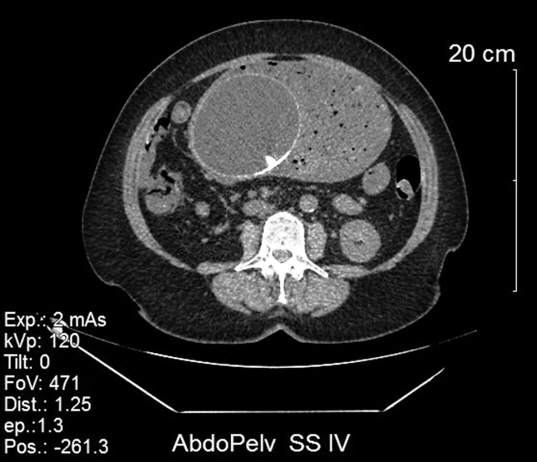
Fig. 1. A rare complication after gastric balloon: presence of a bezoar with gastric dilatation.
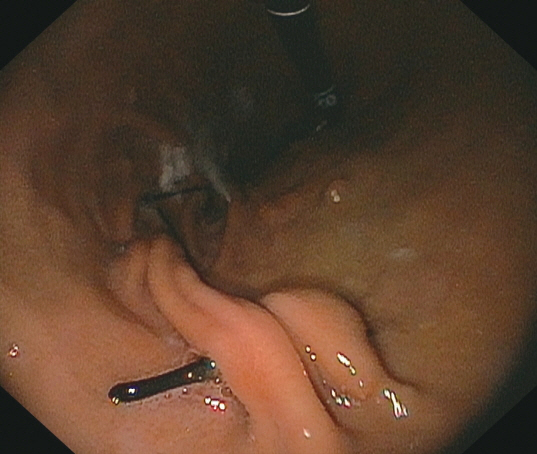
Fig. 2. Endoscopic view of a POSE (USGI Inc.) procedure after 2 years.

Fig. 3. Immediate postoperative X-ray control after an OVERSTITCH (Apollo Endosurgery Inc.) procedure.

Fig. 4. Endoscopic view after surgical gastric plication.
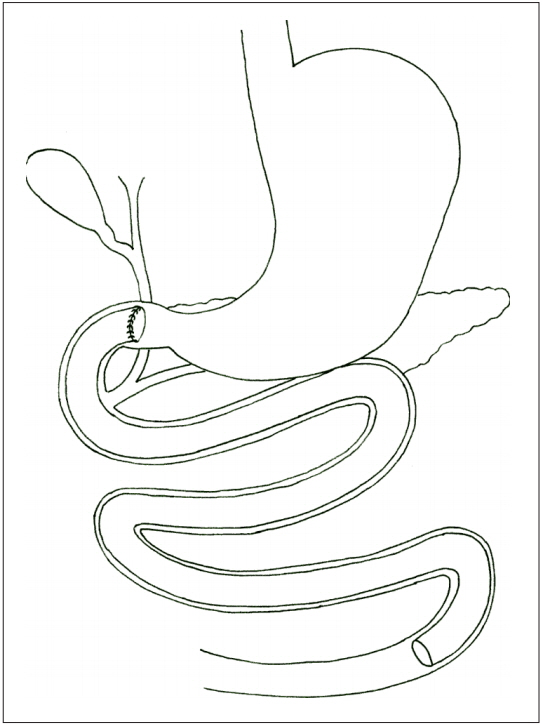
Fig. 5. Endo-duodeno-jejunal bypass.
Reference
-
1. ASGE Bariatric Endoscopy Task Force and ASGE Technology Committee, Abu Dayyeh BK, Kumar N, et al. ASGE Bariatric Endoscopy Task Force systematic review and meta-analysis assessing the ASGE PIVI thresholds for adopting endoscopic bariatric therapies. Gastrointest Endosc. 2015; 82:425–438. e5.
Article2. Busetto L, Dixon J, De Luca M, Shikora S, Pories W, Angrisani L. Bariatric surgery in class I obesity: a position statement from the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO). Obes Surg. 2014; 24:487–519.3. Brooks J, Srivastava ED, Mathus-Vliegen EM. One-year adjustable intragastric balloons: results in 73 consecutive patients in the U.K. Obes Surg. 2014; 24:813–819.
Article4. Ponce J, Quebbemann BB, Patterson EJ. Prospective, randomized, multicenter study evaluating safety and efficacy of intragastric dual-balloon in obesity. Surg Obes Relat Dis. 2013; 9:290–295.
Article5. Mion F, Ibrahim M, Marjoux S, et al. Swallowable Obalon(R) gastric balloons as an aid for weight loss: a pilot feasibility study. Obes Surg. 2013; 23:730–733.6. Deviere J, Ojeda Valdes G, Cuevas Herrera L, et al. Safety, feasibility and weight loss after transoral gastroplasty: first human multicenter study. Surg Endosc. 2008; 22:589–598.
Article7. Horgan S, Jacobsen G, Weiss GD, et al. Incisionless revision of post-Roux-en-Y bypass stomal and pouch dilation: multicenter registry results. Surg Obes Relat Dis. 2010; 6:290–295.
Article8. Espinos JC, Turró R, Mata A, et al. Early experience with the Incisionless Operating Platform (IOP) for the treatment of obesity: the Primary Obesity Surgery Endolumenal (POSE) procedure. Obes Surg. 2013; 23:1375–1383.9. Lopez-Nava G, Galvão MP, Bautista-Castaño I, Jimenez-Baños A, Fernandez-Corbelle JP. Endoscopic sleeve gastroplasty: how I do it? Obes Surg. 2015; 25:1534–1538.
Article10. Sullivan S, Stein R, Jonnalagadda S, Mullady D, Edmundowicz S. Aspiration therapy leads to weight loss in obese subjects: a pilot study. Gastroenterology. 2013; 145:1245–1252. e1-5.
Article11. de Jonge C, Rensen SS, Verdam FJ, et al. Endoscopic duodenal-jejunal bypass liner rapidly improves type 2 diabetes. Obes Surg. 2013; 23:1354–1360.
Article12. Mathus-Vliegen EM, de Groot GH. Fasting and meal-induced CCK and PP secretion following intragastric balloon treatment for obesity. Obes Surg. 2013; 23:622–633.
Article13. de Jong K, Mathus-Vliegen EM, Veldhuyzen EA, Eshuis JH, Fockens P. Short-term safety and efficacy of the Trans-oral Endoscopic Restrictive Implant System for the treatment of obesity. Gastrointest Endosc. 2010; 72:497–504.
Article14. Verlaan T, Paulus GF, Mathus-Vliegen EM, et al. Endoscopic gastric volume reduction with a novel articulating plication device is safe and effective in the treatment of obesity (with video). Gastrointest Endosc. 2015; 81:312–320.
Article15. Marinos G, Eliades C, Muthusamy V, et al. First clinical experience with the transpyloric shuttle device, a non-surgical endoscopic treatment for obesity: results from a 3-month and a 6-month study. In : Proceedings of the SAGES 2013; 2013 Apr 17-20; Baltimore, MD, USA. Los Angeles, CA: SAGES;2013.16. Sauer N, Rösch T, Pezold J, et al. A new endoscopically implantable device (SatiSphere) for treatment of obesity: efficacy, safety, and metabolic effects on glucose, insulin, and GLP-1 levels. Obes Surg. 2013; 23:1727–1733.17. Emerging Technologies and Clinical Issues Committees of the ASMBS. American Society for Metabolic and Bariatric Surgery Position Statement on emerging endosurgical interventions for treatment of obesity. Surg Obes Relat Dis. 2009; 5:297–298.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Currently Available Non-Balloon Devices
- Endoscopic Accessories Used for More Advanced Endoluminal Therapeutic Procedures
- Role of Restrictive Endoscopic Procedures in Obesity Treatment
- The Effect of Bariatric Surgery and Endoscopic Procedures on Gastroesophageal Reflux Disease
- Endoscopic Bariatric Therapy for Obesity and Metabolic Syndrome
