Clin Endosc.
2018 Sep;51(5):416-419. 10.5946/ce.2018.143.
Currently Available Non-Balloon Devices
- Affiliations
-
- 1Department of Internal Medicine, Hanyang University Hospital, Seoul, Korea. alwayshang@hanyang.ac.kr
- KMID: 2427713
- DOI: http://doi.org/10.5946/ce.2018.143
Abstract
- Obesity and metabolic syndrome are known to have an impact on the economy. Obesity and metabolic syndrome affect about 40% population in the America alone, and with about 400 million obese adults in the world, obesity is a global concern. Moreover, the prevalence of overweight children is increasing. Bariatric surgery remains the gold standard for the treatment of obesity; however, endoscopic approaches may have a significant role in the management of metabolic syndrome and obesity. Until recently, many endoscopic methods have been introduced; however, few methods are used in practice, whereas others are under experimental research. Endoscopists have an important role in the treatment of obesity because endoscopic therapies have demonstrated their safety and efficacy over the past few years. Endoscopic bariatric therapies can be categorized as follows: space occupying, malabsorption, and gastric volume reduction. In this review, we summarize the currently available non-balloon type endoscopic procedure.
Keyword
Figure
-

Fig. 1. Endoscopic sleeve gastroplasty, a restrictive procedure to decrease the intraluminal volume with endoscopic suturing for gastric remodeling.
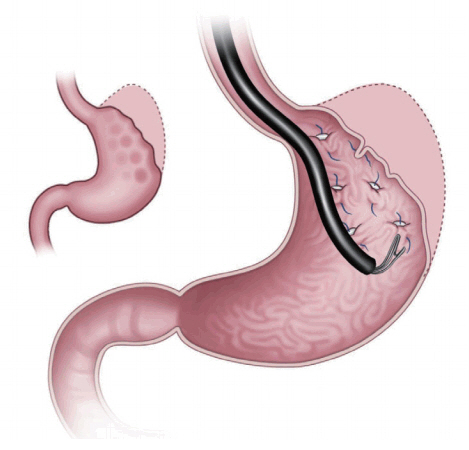
Fig. 2. Primary obesity surgery endoluminal procedure. This procedure facilitates tissue approximation with surrounding tissue through full-thickness stitches.
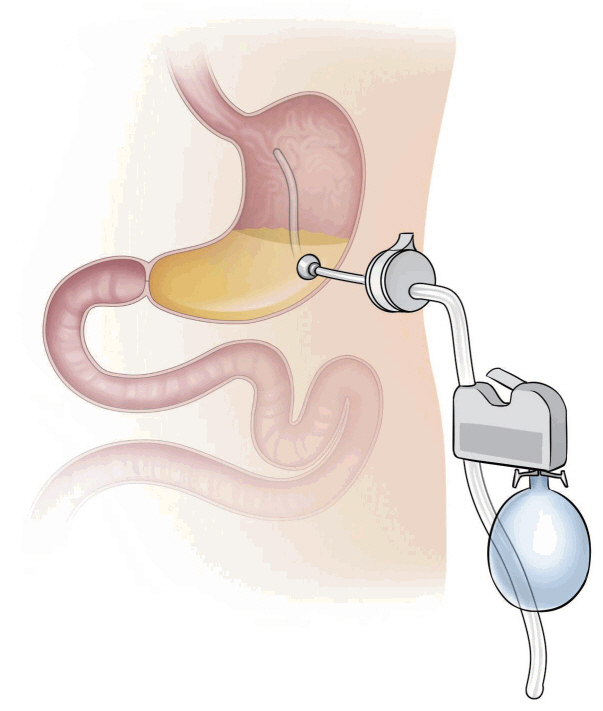
Fig. 3. Aspiration therapy. AspireAssist® consists of a percutaneous endoscopic gastrostomy tube for aspiration of gastric food, a valve located in the skin, and a device for flushing and aspiration.
Reference
-
1. Lee HL. Role of restrictive endoscopic procedures in obesity treatment. Clin Endosc. 2017; 50:17–20.
Article2. Yoo IK, Chun HJ, Jeen YT. Gastric perforation caused by an intragastric balloon: endoscopic findings. Clin Endosc. 2017; 50:602–604.
Article3. Kumar N. Weight loss endoscopy: development, applications, and current status. World J Gastroenterol. 2016; 22:7069–7079.
Article4. Fujii LL, Bonin EA, Baron TH, Gostout CJ, Wong Kee Song LM. Utility of an endoscopic suturing system for prevention of covered luminal stent migration in the upper GI tract. Gastrointest Endosc. 2013; 78:787–793.
Article5. Kumar N, Thompson CC. A novel method for endoscopic perforation management by using abdominal exploration and full-thickness sutured closure. Gastrointest Endosc. 2014; 80:156–161.
Article6. Kumar N, Lopez-Nava G, Sahdala HNP, et al. Endoscopic sleeve gastroplasty: multicenter weight loss results. Gastroenterology. 2015; 148(4 Suppl 1):S–179.7. Lopez-Nava G, Galvao M, Bautista-Castaño I, Fernandez-Corbelle JP, Trell M. Endoscopic sleeve gastroplasty with 1-year follow-up: factors predictive of success. Endosc Int Open. 2016; 4:E222–E227.
Article8. Abu Dayyeh BK, Acosta A, Camilleri M, et al. Endoscopic sleeve gastroplasty alters gastric physiology and induces loss of body weight in obese individuals. Clin Gastroenterol Hepatol. 2017; 15:37–43. e1.9. Sharaiha RZ, Kedia P, Kumta N, et al. Initial experience with endoscopic sleeve gastroplasty: technical success and reproducibility in the bariatric population. Endoscopy. 2015; 47:164–166.
Article10. López-Nava G, Bautista-Castaño I, Jimenez A, de Grado T, Fernandez-Corbelle JP. The primary obesity surgery endolumenal (POSE) procedure: one-year patient weight loss and safety outcomes. Surg Obes Relat Dis. 2015; 11:861–865.
Article11. Espinós JC, Turró R, Mata A, et al. Early experience with the Incisionless Operating Platform™ (IOP) for the treatment of obesity: the primary obesity surgery endolumenal (POSE) procedure. Obes Surg. 2013; 23:1375–1383.12. Sullivan S, Edmundowicz SA, Thompson CC. Endoscopic bariatric and metabolic therapies: new and emerging technologies. Gastroenterology. 2017; 152:1791–1801.
Article13. Sullivan S, Stein R, Jonnalagadda S, Mullady D, Edmundowicz S. Aspiration therapy leads to weight loss in obese subjects: a pilot study. Gastroenterology. 2013; 145:1245–1252. e1-e5.
Article14. Thompson CC, Abu Dayyeh BK, Kushner R, et al. Percutaneous gastrostomy device for the treatment of Class II and Class III obesity: results of a randomized controlled trial. Am J Gastroenterol. 2017; 112:447–457.
Article15. Machytka E, Turro R, Huberty V, et al. Aspiration therapy in super obese patients - pilot trial. Gastroenterology. 2016; 150:S822–S823.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Role of Distal Protection Devices for Cardiovascular Intervention
- Clinical Application of a New Balloon Dissector
- Endovascular Repair Using Suture-Mediated Closure Devices and Balloon Tamponade following Inadvertent Subclavian Artery Catheterization with Large-Caliber Hemodialysis Catheter
- Does Single Balloon Enteroscopy Have Similar Efficacy and Endoscopic Performance Compared with Double Balloon Enteroscopy?
- Experience in High Speed Rotational Coronary Atherectomy
