Improving Conventional or Low Dose Metronomic Chemotherapy with Targeted Antiangiogenic Drugs
- Affiliations
-
- 1Sunnybrook Research Institute, Sunnybrook Health Sciences Centre and the University of Toronto, Toronto, Canada. Robert.kerbel@sri.utoronto.ca
Abstract
- One of the most significant developments in medical oncology practice has been the approval of various antiangiogenic drugs for the treatment of a number of different malignancies. These drugs include bevacizumab (Avastin(R)), the anti-VEGF monoclonal antibody. Thus far, bevacizumab appears to induce clinical benefit in patients who have advanced metastatic disease only or primarily when it is combined with conventional chemotherapy. The reasons for the chemo-enhancing effects of bevacizumab are unknown, and this is a subject that we have been actively studying along with additional ways that antiangiogenic drugs may be combined with chemotherapy. In this respect, we have focused much of our effort on metronomic low dose chemotherapy. We have been studying the hypothesis that some chemotherapy drugs at maximum tolerated doses or other cytotoxic-like drugs such as acute "vascular disrupting agents" (VDAs) can cause an acute mobilization of proangiogenic cells from the bone marrow which home to and colonize the treated tumors, thus accelerating their recovery. These cells include endothelial progenitor cells. This systemic process can be largely blocked by a targeted antiangiogenic drug, e.g. anti-VEGFR-2 antibodies. In addition, metronomic chemotherapy, i.e., close regular administration of chemotherapy drugs at low non-toxic doses with no breaks, over prolonged periods of time not only prevents the acute CEP bone marrow response, but can even target the cells. This potential antiangiogenic effect of metronomic chemotherapy can also be boosted by combination with a targeted antiangiogenic agent. Treatment combinations of metronomic chemotherapy and an antiangiogenic drug have moved into phase II clinical trial testing with particularly encouraging results thus far reported in metastatic breast and recurrent ovarian cancer. Oral chemotherapy drugs such as cyclophosphamide (CTX), methotrexate are the main chemotherapeutics used for such trials. Oral 5-FU prodrugs such as UFT would also appear to be highly suitable based on long term adjuvant therapy studies in patients. Recent preclinical results using metronomic cyclophosphamide and metronomic UFT in models of advanced metastatic breast cancer suggest that this type of combination might be particularly promising for metronomic chemotherapy in this indication, particularly when combined with a targeted antiangiogenic drug.
Keyword
MeSH Terms
-
Antibodies
Bevacizumab
Bone Marrow
Breast
Breast Neoplasms
Colon
Cyclophosphamide
Drug Therapy*
Fluorouracil
Humans
Maximum Tolerated Dose
Medical Oncology
Methotrexate
Neoplasm Metastasis
Ovarian Neoplasms
Prodrugs
Stem Cells
Vascular Endothelial Growth Factor A
Antibodies
Cyclophosphamide
Fluorouracil
Methotrexate
Prodrugs
Vascular Endothelial Growth Factor A
Figure
-
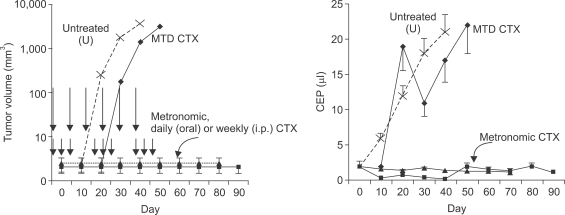
Fig. 1 Differential effects of maximum tolerated dose cyclophosphamide (MTD CTX) versus metronomic low dose chemotherapy on tumor growth (upper panel) or levels of circulating endothelial progenitor cells (CEPs) in peripheral blood of mice (bottom panel). NOD-SCID mice were injected with a human (Granta) lymphoma cells, subcutaneously, and established tumors were then treated with three different forms of CTX, or left untreated. MTD CTX was given in successive 6-day cycles where the drug was injected at 150 mg/kg every other day (shorter vertical arrows) separated by 2-week break periods. The metronomic regimens consisted of either daily continuous administration through the drinking water at an approximate dose of 20 mg/kg per day or weekly intraperitoneal/bolus injections of the drug of 150 mg/kg. Note the far greater anti-tumor efficacy of the two metronomic regimens compared to the conventional and more toxic MTD regimen. The bottom panel illustrates the observation of increasing levels of CEPs in untreated tumor bearing mice with progressive increase in tumor volume. However, when tumor bearing mice are treated with a course of MTD CTX there is an initial decline in CEPs which is then followed by a marked rebound during the drug-free break periods. In contrast, the two different metronomic regimens caused a sustained suppression of CEPs throughout the course of therapy. Taken from Bertolini et al (18) and reproduced with permission of the authors.
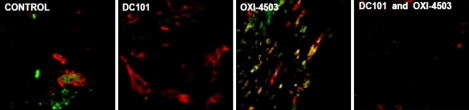
Fig. 2 Acute homing of bone marrow derived circulating cells (including endothelial progenitor cells) to tumors shortly after tumor bearing mice are treated with a single injection of a vascular disrupting agent (VDA) called OXi-4503. Lewis Lung carcinoma cells were grown in syngeneic C57/Bl6 mice that had previously been lethally irradiated and reconstituted with syngeneic GFP-positive bone marrow cells. Note low levels of GFP-positive cells in tumors from untreated (control) or DC101 treated mice. However, 72 hours after OXi-4503 treatment a pronounced GFP cell colonization is evident, a process which can be prevented by prior treatment with DC101, an anti-VEGFR-2 monoclonal neutralizing antibody. The CEP homing phenomenon was shown to contribute to tumor angiogenesis and tumor growth at the viable tumor rim which characteristically remains after VDA treatment. Taken from Shaked et al (26) with permission of the authors.
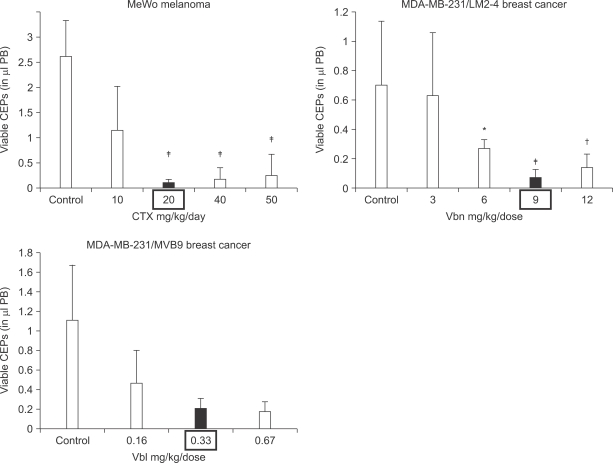
Fig. 3 Using circulating endothelial progenitor cells (CEPs) in peripheral blood as a surrogate biomarker for establishing the optimal biologic dose (OBD) for metronomic chemotherapy. Tumor bearing mice were treated with cyclophosphamide (CTX) daily for a week, or vinorelbine (Vbn) or vinblastine (Vbl) twice a week by intraperitoneal injection at the indicated doses and then viable CEPs assessed in peripheral blood samples by four color flow cytometry. In addition, anti-tumor effects and host toxicity (e.g. loss of body weight) were assessed in separate experiments, and correlated with the CEP results. The OBDs for the three drugs are highlighted in boxes, e.g. 20 mg/kg/day for CTX, 9 mg/kg/dose for Vbn and 0.33 mg/kg/dose for Vbl, which coincide with the nadir of CEPs detected and maximal anti-tumor activity along with acceptable or no toxicity. All tumors tested were of human origin, and were described in Shaked et al (29). Significant differences from control are present by *p>0.05, †0.05>p>0.01 and ‡p<0.01.
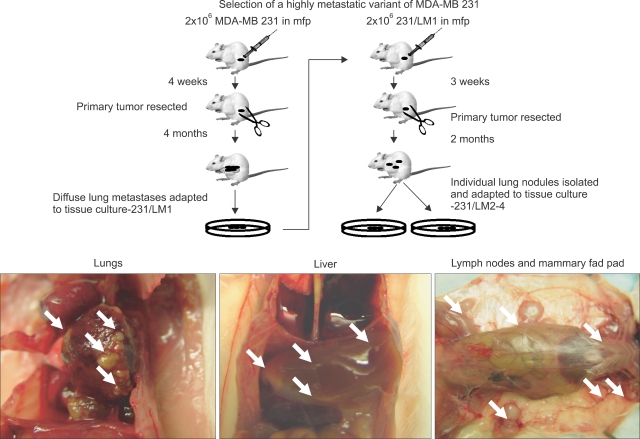
Fig. 4 Procedure used for selecting the highly metastatic MDA-MB-231 human breast cancer variant, 231/LM2-4. MDA-MB-231 cells were injected into the mammary fat pads (MFPs) of SB-17 SCID mice, i.e., orthotopically injected. The 231/LM2-4 variant was obtained subsequent to two rounds of lung metastasis selection in mice, after surgical removal of the primary orthotopically transplanted tumor, as explained in detail in the text and outlined in the diagram. Primary tumors were removed when volumes reached approximately 400 mm2. Six weeks later mice were sacrificed and examined for the presence of macrometastases in the lungs, liver, lymph nodes and MFPs. Blue arrows indicate typical location of metastatic lesions. The sequence for the selection strategy was as follows: i) 2×106 MDA-MB 231 cells were injected into the MFP of adult 6~8 week old female CB17 SCID mice; ii) four weeks later the primary tumor was resected fully by surgery when the tumor volumes were 300~500 mm3; iii) at monthly intervals, groups of mice were sacrificed and checked for presence of metastases in the lungs and full blown diffuse metastatic spread was observed in the mice after 4 months; iv) the whole set of lungs from one mouse were adapted to tissue culture and grown for 3 passages to derive a line referred to as 231/LM1; v) 2X106 231/LM1 cells were injected into the MFP of adult 6~8 week old female CB17 SCID mice; vi) approximately 3 weeks later the primary tumor was resected when the tumor volume was 300~500 mm3; vii) again, at monthly intervals, groups of mice were sacrificed and checked for metastases in the lungs; 2 months after resection of the primary tumor, mice were observed to have numerous macroscopic lung nodules with some spilling into the pleural cavity; viii) several individual lung nodules were isolated and adapted to tissue culture to derive established lines, one of which 231/LM2-4, was selected for in vivo studies. Overall, this selection procedure took almost nine months to complete. Genotypic analysis of MDA-MB-231 and the 231/LM2-4 variant verified their human origin and lineage relationship (data not shown). Surgical resection of primary tumors was carried out by skin incision and carefully clearing all tumor tissue away from surrounding connective tissue. Weekly weight assessment was used as a surrogate marker for toxicity. The mice were sacrificed when tumor sizes reached 1.7 cm3. The bottom panel shows a photograph of the pattern of metastatic spread that can be attained within one month using the LM2.4 variant after surgical excision of the primary tumor. Taken from Munoz et al (31) with permission of the authors.
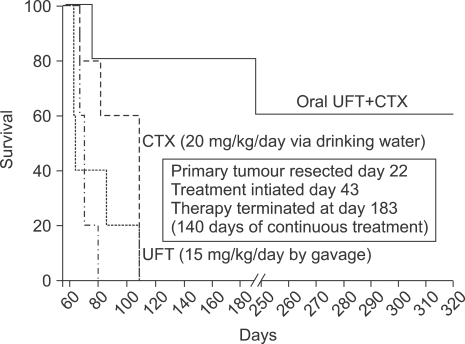
Fig. 5 Chronic combination oral metronomic low-dose CTX and UFT prolongs survival of mice with advanced metastatic disease. 231/LM2-4 human breast metastatic variant cells were orthotopically injected into the MFPs of 6~8 week old CB17 SCID mice. When tumors reached volumes of approximately 200 mm3, treatment with either vehicle control, or 15 mg/kg/day UFT by gavage, or 20 mg/kg/day CTX through the drinking water, or a combination of CTX and UFT treatments was initiated. Tumors were measured weekly and tumor volume was plotted accordingly. Arrow indicates time of initiation of treatment. When tumors reached 400 mm3 (which took approximately 3 weeks) primary tumors were surgically removed. Treatment with vehicle control, 15 mg/kg/day UFT by gavage, 20 mg/kg/day CTX through the drinking water, or the daily combination of metronomic UFT and CTX, were initiated 3 weeks after surgery on a daily non-stop basis. For example, the duration of the therapy was 140 days, and was initiated on day 43, 3 weeks after surgery, with termination at day 183. Mice were monitored frequently according to the institutional guidelines. A Kaplan-Meier survival curve was plotted accordingly for all treated group, as indicated in the figure. n=7~9 mice/group. Taken from Munoz et al (31) with permission of the authors.
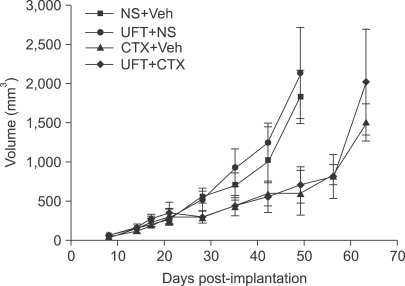
Fig. 6 Effect of metronomic cyclophosphamide (CTX) or metronomic UFT, or the two drugs together on the growth of orthotopically implanted MDA-MB-231 LM2.4 human breast cancer carcinoma. Treatment was started when tumors in the mammary fat pad attained a size of about 200 mm3 and was maintained until mice had to be sacrificed. The doses and schedules used are as for Fig. 5. NS: normal saline, Veh: vehicle control for UFT. Note lack of effect of UFT alone on primary tumor volumes or when added to metronomic CTX. However, metronomic UFT was found to have a potent local anti-invasive effect on the primary tumors and also inhibited development of microscopic metastases as described by Munoz et al (31). Taken from Munoz et al (31) with permission of the authors.
Reference
-
1. Ferrara N, Kerbel RS. Angiogenesis as a therapeutic target. Nature. 2005; 438:967–974. PMID: 16355214.
Article2. Kerbel RS. Antiangiogenic therapy: a universal chemosensitization strategy for cancer? Science. 2006; 312:1171–1175. PMID: 16728631.
Article3. Kerbel RS, Kamen BA. Antiangiogenic basis of low-dose metronomic chemotherapy. Nature Rev Cancer. 2004; 4:423–436. PMID: 15170445.4. Miller KD, Sweeney CJ, Sledge GW Jr. Redefining the target: chemotherapeutics as antiangiogenics. J Clin Oncol. 2001; 19:1195–1206. PMID: 11181686.
Article5. Browder T, Butterfield CE, Kraling BM, Marshall B, O'Reilly MS, Folkman J. Antiangiogenic scheduling of chemotherapy improves efficacy against experimental drug-resistant cancer. Cancer Res. 2000; 60:1878–1886. PMID: 10766175.6. Colleoni M, Rocca A, Sandri MT, Zorzino L, Masci G, Nole F, et al. Low dose oral methotrexate and cyclophosphamide in metastatic breast cancer: antitumor activity and correlation with vascular endothelial growth factor levels. Ann Oncol. 2002; 13:73–80. PMID: 11863115.7. Emmenegger U, Man S, Shaked Y, Francia G, Wong JW, Hicklin DJ, et al. A comparative analysis of low dose metronomic cyclophosphamide reveals absent or low grade toxicity on tissues highly sensitive to the toxic effects of maximum tolerated dose regimens. Cancer Res. 2004; 64:3994–4000. PMID: 15173013.8. Klement G, Baruchel S, Rak J, Man S, Clark K, Hicklin D, et al. Continuous low-dose therapy with vinblastine and VEGF receptor-2 antibody induces sustained tumor regression without overt toxicity. J Clin Invest. 2000; 105:R15–R24. PMID: 10772661.
Article9. Pietras K, Hanahan D. A multitargeted, metronomic, and maximum-tolerated dose "chemo-switch" regimen is antiangiogenic, producing objective responses and survival benefit in a mouse model of cancer. J Clin Oncol. 2005; 23:939–952. PMID: 15557593.
Article10. du Manoir JM, Francia G, Man S, Mossoba M, Medin JA, Viloria-Petit A, et al. Strategies for delaying or treating in vivo acquired resistance to trastuzumab (Herceptin®) in human breast cancer xenografts. Clin Cancer Res. 2006; 12:904–916. PMID: 16467105.11. Hermans IF, Chong TW, Palmowski MJ, Harris AL, Cerundolo V. Synergistic effect of metronomic dosing of cyclophosphamide combined with specific antitumor immunotherapy in a murine melanoma model. Cancer Res. 2003; 63:8408–8413. PMID: 14679003.12. Bottini A, Generali D, Brizzi MP, Fox SB, Bersiga A, Bonardi S, et al. Randomized phase II trial of letrozole and letrozole plus low-dose metronomic oral cyclophosphamide as primary systemic treatment in elderly breast cancer patients. J Clin Oncol. 2006; 24:3623–3628. PMID: 16877730.
Article13. Bocci G, Tuccori M, Emmenegger U, Liguori V, Kerbel RS, Del Tacca M. Cyclophosphamide-methotrexate "metronomic" chemotherapy for the palliative treatment of metastatic breast cancer. A comparative pharmacoeconomic evaluation. Ann Oncol. 2004; 16:1243–1252. PMID: 15905308.
Article14. Kato H, Ichinose Y, Ohta M, Hata E, Tsubota N, Tada H, et al. A randomized trial of adjuvant chemotherapy with uraciltegafur for adenocarcinoma of the lung. N Engl J Med. 2004; 350:1713–1721. PMID: 15102997.
Article15. Tannock IF. Population kinetics of carcinoma cells, capillary endothelial cells, and fibroblasts in a transplanted mouse mammary tumor. Cancer Res. 1970; 30:2470–2476. PMID: 4097429.16. Eberhard A, Kahlert S, Goede V, Hemmerlein B, Plate KH, Augustin HG. Heterogeneity of angiogenesis and blood vessel maturation in human tumors: implications for antiangiogenic tumor therapies. Cancer Res. 2000; 60:1388–1393. PMID: 10728704.17. Kerbel RS. Inhibition of tumor angiogenesis as a strategy to circumvent acquired resistance to anti-cancer therapeutic agents. Bioessays. 1991; 13:31–36. PMID: 1722975.
Article18. Bertolini F, Paul S, Mancuso P, Monestiroli S, Gobbi A, Shaked Y, et al. Maximum tolerable dose and low-dose metronomic chemotherapy have opposite effects on the mobilization and viability of circulating endothelial progenitor cells. Cancer Res. 2003; 63:4342–4346. PMID: 12907602.19. Furstenberger G, von Moos R, Lucas R, Thurlimann B, Senn HJ, Hamacher J, et al. Circulating endothelial cells and angiogenic serum factors during neoadjuvant chemotherapy or primary breast cancer. Br J Cancer. 2006; 94:524–531. PMID: 16450002.20. Hudis CA. Clinical implications of antiangiogenic therapies. Oncology. 2005; 19:26–31. PMID: 15934500.21. Asahara T, Murohara T, Sullivan A, Silver M, van der Zee R, Li T, et al. Isolation of putative progenitor endothelial cells for angiogenesis. Science. 1997; 275:964–967. PMID: 9020076.
Article22. Shaked Y, Bertolini F, Man S, Rogers MS, Cervi D, Foutz T, et al. Genetic heterogeneity of the vasculogenic phenotype parallels angiogenesis: implications for cellular surrogate marker analysis of antiangiogenesis. Cancer Cell. 2005; 7:101–111. PMID: 15652753.23. Bertolini F, Shaked Y, Mancuso P, Kerbel RS. The multifaceted circulating endothelial cell in cancer: from promiscuity to surrogate marker and target identification. Nature Rev Cancer. 2006; 6:835–845. PMID: 17036040.24. Garcia-Barros M, Paris F, Cordon-Cardo C, Lyden D, Rafii S, Haimovitz-Friedman A, et al. Tumor response to radiotherapy regulated by endothelial cell apoptosis. Science. 2003; 300:1155–1159. PMID: 12750523.
Article25. Spring H, Schuler T, Arnold B, Hammerling GJ, Ganss R. Chemokines direct endothelial progenitors into tumor neovessels. Proc Natl Acad Sci USA. 2005; 102:18111–18116. PMID: 16326806.
Article26. Shaked Y, Ciarrocchi A, Franco M, Lee CR, Man S, Cheung AM, et al. Therapy-induced acute recruitment of circulating endothelial progenitor cells to tumors. Science. 2006; 313:1785–1787. PMID: 16990548.
Article27. Tozer GM, Kanthou C, Baguley BC. Disrupting tumour blood vessels. Nat Rev Cancer. 2005; 5:423–435. PMID: 15928673.
Article28. Ghiringhelli F, Menard C, Puig PE, Ladoire S, Roux S, Martin F, et al. Metronomic cyclophosphamide regimen selectively depletes CD4(+)CD25(+) regulatory T cells and restores T and NK effector functions in end stage cancer patients. Cancer Immunol Immunother. 2006; 56:641–648. PMID: 16960692.
Article29. Shaked Y, Emmengger U, Man S, Cervi D, Bertolini F, Ben-David Y, et al. The optimal biological dose of metronomic chemotherapy regimens is associated with maximum antiangiogenic activity. Blood. 2005; 106:3058–3061. PMID: 15998832.30. Ng SS, Sparreboom A, Shaked Y, Lee C, Man S, Desai N, et al. Influence of formulation vehicle on metronomic taxane chemotherapy: albumin-bound versus cremophor EL-based paclitaxel. Clin Cancer Res. 2006; 12:4331–4338. PMID: 16857808.
Article31. Munoz R, Man S, Shaked Y, Lee C, Wong J, Francia G, et al. Highly efficacious non-toxic treatment for advanced metastatic breast cancer using combination UFT-cyclophosphamide metronomic chemotherapy. Cancer Res. 2006; 66:3386–3391. PMID: 16585158.32. Mancuso P, Colleoni M, Calleri A, Orlando L, Maisonneuve P, Pruneri G, et al. Circulating endothelial cell kinetics and viability predict survival in breast cancer patients receiving metronomic chemotherapy. Blood. 2006; 108:452–459. PMID: 16543470.33. Man S, Bocci G, Francia G, Green S, Jothy S, Bergers G, et al. Antitumor and anti-angiogenic effects in mice of low-dose (metronomic) cyclophosphamide administered continuously through the drinking water. Cancer Res. 2002; 62:2731–2735. PMID: 12019144.34. Kerbel RS. Human tumor xenografts as predictive preclinical models for anticancer drug activity in humans: better than commonly perceived - but they can be improved. Cancer Biol Ther. 2003; 2:S134–S139. PMID: 14508091.35. Man S, Munoz R, Kerbel RS. On the development of models in mice of advanced visceral metastatic disease for anti-cancer drug testing. Cancer Metastasis Rev. 2007; epub ahead of print.
Article36. Rocca A, Dellapasqua S, Pietri E. Metronomic chemotherapy with capecitabine and oral cyclophosphamide in combination with bevacizumab in metastatic breast cancer (mbc): evidence of activity of an antianigogenic treatment. Proc Am Soc Clin Oncol. 2007; #11501(2007) (Abstract).37. Buckstein R, Crump M, Shaked Y, Nayar R, Foden C, Turner R, et al. High dose celecoxib and metronomic 'low dose' cyclophosphamide is effective and safe therapy in patients with relapsed and refractory aggressive histology NHL. Clin Cancer Res. 2006; 12:5190–5198. PMID: 16951238.38. Garcia AA, Hirte H, Fleming G, Yang D, Tsao-Wei DD, Roman L, et al. Phase II clinical trial of bevacizumab and low dose metronomic oral cyclophosphamide in recurrent ovarian cancer. A study of the California, Chicago and Princess Margaret Hospital Phase II Consortia. J Clin Oncol. 2007; in press.39. Glode LM, Crighton F, Barqawi A, Kerbel RS, Berman C, Crawford D. Metronomic therapy with cyclophosphamide and dexamethasone for prostate cancer. Cancer. 2003; 98:1643–1648. PMID: 14534880.40. Orlando L, Cardillo A, Rocca A, Balduzzi A, Ghisini R, Peruzzotti G, et al. Prolonged clinical benefit with metronomic chemotherapy in patients with metastatic breast cancer. Anticancer Drugs. 2006; 17:961–967. PMID: 16940806.
Article41. Vogt T, Hafner C, Bross K, Bataille F, Jauch KW, Berand A, et al. Antiangiogenetic therapy with pioglitazone, rofecoxib, and metronomic trofosfamide in patients with advanced malignant vascular tumors. Cancer. 2003; 98:2251–2256. PMID: 14601096.
Article42. Kong DS, Lee JI, Kim WS, Son MJ, Lim dH, Kim ST, et al. A pilot study of metronomic temozolomide treatment in patients with recurrent temozolomide-refractory glioblastoma. Oncol Rep. 2006; 16:1117–1121. PMID: 17016602.
Article43. Reichle A, Bross K, Vogt T, Bataille F, Wild P, Berand A, et al. Pioglitazone and rofecoxib combined with angiostatically scheduled trofosfamide in the treatment of far-advanced melanoma and soft tissue sarcoma. Cancer. 2004; 101:2247–2256. PMID: 15470711.
Article44. Buckstein R, Kerbel RS, Shaked Y, Nayar R, Foden C, Turner R, et al. High-dose celecoxib and metronomic "low-dose" cyclophosphamide is an effective and safe therapy in patients with relapsed and refractory aggressive histology non-Hodgkin's lymphoma. Clin Cancer Res. 2006; 12:5190–5198. PMID: 16951238.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two cases of advanced hepatocellular carcinoma achieving a complete response with metronomic chemotherapy via the hepatic artery
- Can metronomic chemotherapy be an alternative to sorafenib in advanced hepatocellular carcinoma?
- Advanced ovarian cancer: what should be the standard of care?
- Efficacy and safety of metronomic chemotherapy for patients with advanced primary hepatocellular carcinoma with major portal vein tumor thrombosis
- Commentary on “Metronomic S-1 Adjuvant Chemotherapy Improves Survival in Patients with Locoregionally Advanced Nasopharyngeal Carcinoma”
