No Concentration Decrease of House Dust Mite Allergens With Rising Altitude in Alpine Regions
- Affiliations
-
- 1Institute of Ecomedicine, Paracelsus Medical University, Salzburg, Austria. arnulf.hartl@pmu.ac.at
- 2Institute of Physiology and Pathophysiology, Paracelsus Medical University, Salzburg, Austria.
- 3Department of Molecular Biology, University of Salzburg, Salzburg, Austria.
- KMID: 2165914
- DOI: http://doi.org/10.4168/aair.2016.8.4.312
Abstract
- PURPOSE
Several studies over the past 4 decades have indicated a significant reduction in house dust mite (HDM) and HDM allergen concentration in areas higher than 1,500 m above sea level. These have served as basis of allergen avoidance therapies for HDM allergy and asthma. However, modern construction techniques used in the insulation, heating, and glazing of buildings as well as global warming have changed the environmental parameters for HDM living conditions. The present study revisits the paradigm of decreasing HDM allergen concentrations with increasing altitude in the alpine region of Germany and Austria.
METHODS
A total of 122 dust samples from different abodes (hotels, privates and mountain huts) at different altitudes (400-2,600 m) were taken, and concentrations of HDM allergens were analyzed. Humidity and temperature conditions, and numerous indoor environmental parameters such as fine dust, type of flooring, age of building, and frequency of cleaning were determined.
RESULTS
HDM allergen concentrations did not significantly change with increasing altitude or relative humidity. At the level of indoor parameters, correlations could be found for different flooring types and the concentration of HDM allergens.
CONCLUSIONS
In contrast to the widespread view of the relationship between altitude and HDM allergen concentrations, clinically relevant concentrations of HDM allergens could be detected in high-lying alpine regions in Austria and Germany. These results indicate that improvement in conditions of asthmatic patients sensitized against HDMs during a stay at high altitude can no longer be ascribed to decreased levels of HDM allergens, instead, other mechanisms may trigger the beneficial effect.
Keyword
MeSH Terms
Figure
-
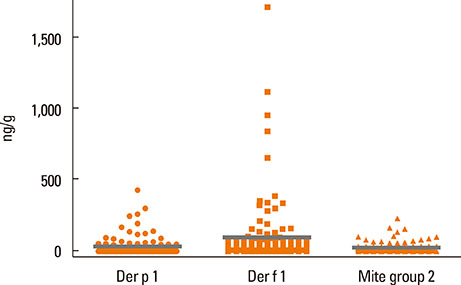
Fig. 1 Total number of allergens: Data shown as distribution of individual allergen concentrations of Der p 1, Der f 1, and Mite group 2 with means (grey lines). n=122 each.
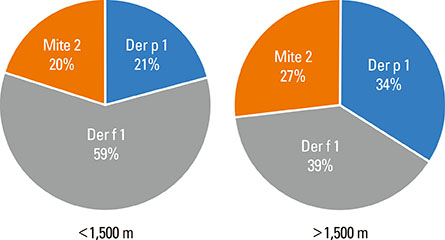
Fig. 2 Percentage of allergen concentrations of Der p 1, Der f 1 and Mite group 2 of the samples taken at 400-1,500 m a.s.l. (n=65) and 1,500-2,600 m a.s.l. (n=57). There are significant higher Der f 1 allergen levels compared to those of Der p 1 (P=0.001) below 1,500 m, but no concentration differences at higher altitude (P=0.689).
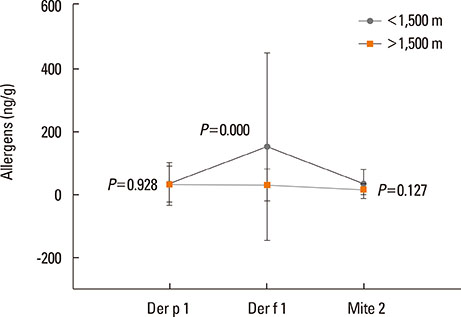
Fig. 3 Allergen concentrations of Der p 1, Der f 1, and Mite group 2 of the samples taken above (n=57) and below 1,500 m a.s.l. (n=65). There are significant lower Der f 1 allergen levels at high altitude compared to allergen levels below 1,500 m a.s.l. (P<0.001). For Der p 1 and Mite 2 allergens, no concentration differences between high and low altitudes could be detected (Der p 1: P=0.928; Mite 2: P=0.127).
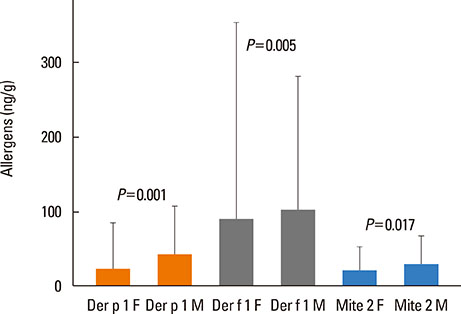
Fig. 4 Comparison of allergen concentrations of the samples taken from floors (F) and mattresses (M) with standard deviations. Allergen concentrations of all 3 HDM allergens were significantly higher in mattresses (Der p 1: P=0.001; Der f 1: P=0.005; Mite group 2: P=0.017).
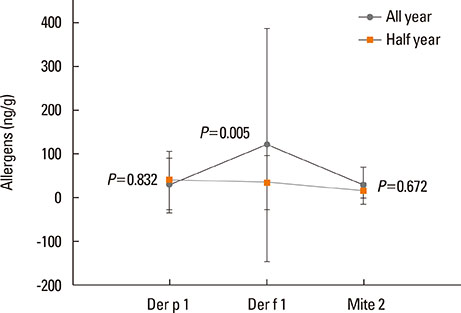
Fig. 5 HDM allergen concentrations in different habitats. Means and standard deviation indicate allergen concentrations given in ng/g of dust of the samples from buildings used year-round (n=85) and from those used only half a year (n=37).
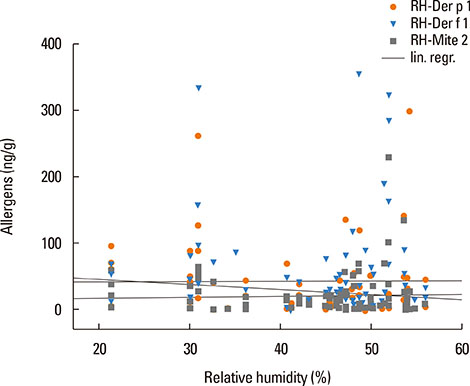
Fig. 6 Relative air humidity (RH) to allergen concentration. The linear regression indicates no correlation between Der p 1, Der f 1, and Mite group 2 allergens with relative air humidity.
Cited by 1 articles
-
House Dust Mite Allergy Under Changing Environments
Nathalie Acevedo, Josefina Zakzuk, Luis Caraballo
Allergy Asthma Immunol Res. 2019;11(4):450-469. doi: 10.4168/aair.2019.11.4.450.
Reference
-
1. Bachert C, Lange B, Virchow JC. Asthma und allergische rhinitis. 1st ed. Stuttgart: Thieme;2005.2. Seo JH, Kim HY, Jung YH, Lee E, Yang SI, Yu HS, et al. Interactions between innate immunity genes and early-life risk factors in allergic rhinitis. Allergy Asthma Immunol Res. 2015; 7:241–248.3. Kim BJ, Lee SY, Kim HB, Lee E, Hong SJ. Environmental changes, microbiota, and allergic diseases. Allergy Asthma Immunol Res. 2014; 6:389–400.4. Gough L, Schulz O, Sewell HF, Shakib F. The cysteine protease activity of the major dust mite allergen Der p 1 selectively enhances the immunoglobulin E antibody response. J Exp Med. 1999; 190:1897–1902.5. Hammad H, Charbonnier AS, Duez C, Jacquet A, Stewart GA, Tonnel AB, et al. Th2 polarization by Der p 1--pulsed monocyte-derived dendritic cells is due to the allergic status of the donors. Blood. 2001; 98:1135–1141.6. Traidl-Hoffmann C, Jakob T, Behrendt H. Determinants of allergenicity. J Allergy Clin Immunol. 2009; 123:558–566.7. Platts-Mills TA. The role of indoor allergens in chronic allergic disease. J Allergy Clin Immunol. 2007; 119:297–302.8. Woodcock A, Custovic A. ABC of allergies. Avoiding exposure to indoor allergens. BMJ. 1998; 316:1075–1078.9. De Alba J, Raemdonck K, Dekkak A, Collins M, Wong S, Nials AT, et al. House dust mite induces direct airway inflammation in vivo: implications for future disease therapy? Eur Respir J. 2010; 35:1377–1387.10. Johnson JR, Wiley RE, Fattouh R, Swirski FK, Gajewska BU, Coyle AJ, et al. Continuous exposure to house dust mite elicits chronic airway inflammation and structural remodeling. Am J Respir Crit Care Med. 2004; 169:378–385.11. Khlgatian SV, Perova NA. Allergens from Dermatophagoides dust mites: origin, antigenic and structural characteristics, and therapeutic agents. Biokhimiia. 1995; 60:218–237.12. Sidenius KE, Hallas TE, Stenderup J, Poulsen LK, Mosbech H. Decay of house-dust mite allergen Der f 1 at indoor climatic conditions. Ann Allergy Asthma Immunol. 2002; 89:34–37.13. de Boer R, van der Hoeven WA, Stapel SO. The decay of house dust mite allergens, Der p I and Der p II, under natural conditions. Clin Exp Allergy. 1995; 25:765–770.14. Platts-Mills TA, Heymann PW, Chapman MD, Hayden ML, Wilkins SR. Cross-reacting and species-specific determinants on a major allergen from Dermatophagoides pteronyssinus and D. farinae: development of a radioimmunoassay for antigen P1 equivalent in house dust and dust mite extracts. J Allergy Clin Immunol. 1986; 78:398–407.15. Grootendorst DC, Dahlén SE, Van Den Bos JW, Duiverman EJ, Veselic-Charvat M, Vrijlandt EJ, et al. Benefits of high altitude allergen avoidance in atopic adolescents with moderate to severe asthma, over and above treatment with high dose inhaled steroids. Clin Exp Allergy. 2001; 31:400–408.16. Huss K, Adkinson NF Jr, Eggleston PA, Dawson C, Van Natta ML, Hamilton RG. House dust mite and cockroach exposure are strong risk factors for positive allergy skin test responses in the Childhood Asthma Management Program. J Allergy Clin Immunol. 2001; 107:48–54.17. Gómez MS, Portus M, Gallego J. Factors influencing the house dust mite population. IV. Altitude Allergol. Allergol Immunopathol (Madr). 1981; 9:123–130.18. Vervloet D, Penaud A, Razzouk H, Senft M, Arnaud A, Boutin C, et al. Altitude and house dust mites. J Allergy Clin Immunol. 1982; 69:290–296.19. Spieksma FT, Zuidema P, Leupen MJ. High altitude and house-dust mites. BMJ. 1971; 1:82–84.20. Menz G, Petri E, Lind P, Virchow C. House dust mite in different altitudes of Grisons. Experientia Suppl. 1987; 51:197–201.21. Charpin D, Birnbaum J, Haddi E, Genard G, Lanteaume A, Toumi M, et al. Altitude and allergy to house-dust mites. A paradigm of the influence of environmental exposure on allergic sensitization. Am Rev Respir Dis. 1991; 143:983–986.22. de Andrade AD, Bartal M, Birnbaum J, Lanteaume A, Charpin D, Vervloet D. House dust mite allergen content in two areas with large differences in relative humidity. Ann Allergy Asthma Immunol. 1995; 74:314–316.23. Menz G. Effect of sustained high altitude on asthma patients. Expert Rev Respir Med. 2007; 1:219–225.24. Gitoho F, Rees P. High altitude and house-dust mites. BMJ. 1971; 3:475.25. Valdivieso R, Iraola V, Pinto H. Presence of domestic mites at an extremely high altitude (4800 m) in Andean Ecuador. J Investig Allergol Clin Immunol. 2009; 19:323–324.26. Valdivieso R, Iraola V, Estupiñán M, Fernández-Caldas E. Sensitization and exposure to house dust and storage mites in high-altitude areas of ecuador. Ann Allergy Asthma Immunol. 2006; 97:532–538.27. Valdivieso R, Estupiñan M, Acosta ME. Asthma and its relation with Dermatophagoides pteronyssinus and Dermatophagoides farinae in Andean altitudes (Quito, Ecuador). J Investig Allergol Clin Immunol. 1997; 7:46–50.28. Blackhall K, Appleton S, Cates CJ. Ionisers for chronic asthma. Cochrane Database Syst Rev. 2003; (3):CD002986.29. Peroni DG, Boner AL, Vallone G, Antolini I, Warner JO. Effective allergen avoidance at high altitude reduces allergen-induced bronchial hyperresponsiveness. Am J Respir Crit Care Med. 1994; 149:1442–1446.30. Peroni DG, Piacentini GL, Costella S, Pietrobelli A, Bodini A, Loiacono A, et al. Mite avoidance can reduce air trapping and airway inflammation in allergic asthmatic children. Clin Exp Allergy. 2002; 32:850–855.31. Valletta EA, Piacentini GL, Del Col G, Boner AL. FEF25-75 as a marker of airway obstruction in asthmatic children during reduced mite exposure at high altitude. J Asthma. 1997; 34:127–131.32. van Velzen E, van den Bos JW, Benckhuijsen JA, van Essel T, de Bruijn R, Aalbers R. Effect of allergen avoidance at high altitude on direct and indirect bronchial hyperresponsiveness and markers of inflammation in children with allergic asthma. Thorax. 1996; 51:582–584.33. Charpin D, Kleisbauer JP, Lanteaume A, Razzouk H, Vervloet D, Toumi M, et al. Asthma and allergy to house-dust mites in populations living in high altitudes. Chest. 1988; 93:758–761.34. Eggleston PA. Improving indoor environments: reducing allergen exposures. J Allergy Clin Immunol. 2005; 116:122–126.35. Arlian LG, Neal JS, Morgan MS, Vyszenski-Moher DL, Rapp CM, Alexander AK. Reducing relative humidity is a practical way to control dust mites and their allergens in homes in temperate climates. J Allergy Clin Immunol. 2001; 107:99–104.36. Dornelas de Andrade A, Birnbaum J, Lanteaume A, Izard JL, Corget P, Artillan MF, et al. Housing and house-dust mites. Allergy. 1995; 50:142–146.37. Cho SH, Reponen T, Bernstein DI, Olds R, Levin L, Liu X, et al. The effect of home characteristics on dust antigen concentrations and loads in homes. Sci Total Environ. 2006; 371:31–43.38. van Strien RT, Gehring U, Belanger K, Triche E, Gent J, Bracken MB, et al. The influence of air conditioning, humidity, temperature and other household characteristics on mite allergen concentrations in the northeastern United States. Allergy. 2004; 59:645–652.39. McCormack MC, Breysse PN, Matsui EC, Hansel NN, Peng RD, Curtin-Brosnan J, et al. Indoor particulate matter increases asthma morbidity in children with non-atopic and atopic asthma. Ann Allergy Asthma Immunol. 2011; 106:308–315.40. Jacquemin B, Schikowski T, Carsin AE, Hansell A, Krämer U, Sunyer J, et al. The role of air pollution in adult-onset asthma: a review of the current evidence. Semin Respir Crit Care Med. 2012; 33:606–619.41. Vernon MK, Wiklund I, Bell JA, Dale P, Chapman KR. What do we know about asthma triggers? A review of the literature. J Asthma. 2012; 49:991–998.42. Sun JL, Shen L, Chen J, Yu JM, Yin J. Mite and booklouse fauna from vacuumed dust samples from beijing. Allergy Asthma Immunol Res. 2014; 6:257–262.43. King EM, Filep S, Smith B, Platts-Mills T, Hamilton RG, Schmechel D, et al. A multi-center ring trial of allergen analysis using fluorescent multiplex array technology. J Immunol Methods. 2013; 387:89–95.44. Richardson G, Eick S, Jones R. How is the indoor environment related to asthma?: literature review. J Adv Nurs. 2005; 52:328–339.45. Charpin D. High altitude and asthma: beyond house dust mites. Eur Respir J. 2012; 40:1320–1321.46. Vervloet D, Bongrand P, Arnaud A, Boutin C, Charpin J. Objective immunological and clinical data observed during an altitude cure at Briançon in asthmatic children allergic to house dust and dermatophagoides (author's transl). Rev Fr Mal Respir. 1979; 7:19–27.47. Karagiannidis C, Hense G, Rueckert B, Mantel PY, Ichters B, Blaser K, et al. High-altitude climate therapy reduces local airway inflammation and modulates lymphocyte activation. Scand J Immunol. 2006; 63:304–310.48. Rijssenbeek-Nouwens LH, Fieten KB, Bron AO, Hashimoto S, Bel EH, Weersink EJ. High-altitude treatment in atopic and nonatopic patients with severe asthma. Eur Respir J. 2012; 40:1374–1380.49. Kim SH, Mun SJ, Han DH, Kim JW, Kim DY, Rhee CS. Three-year follow-up results of sublingual immunotherapy in patients with allergic rhinitis sensitized to house dust mites. Allergy Asthma Immunol Res. 2015; 7:118–123.50. Bielory L, Lyons K, Goldberg R. Climate change and allergic disease. Curr Allergy Asthma Rep. 2012; 12:485–494.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- House dust mite fauna in western Anatolia, Turkey
- Correlation between House Dust Mite Allergen Concentrations in Scalp Dander and Clinical Severity of Atopic Dermatitis in Children
- Food and house dust mite allergens in children with atopic dermatitis
- Repellent effect of Mate tea and Jasmine tea against house dust mites (Dermatophagoides farinae and D. pteronyssinus)
- Review on Ecology of House Dust Mites in Korea and Suggestion of a Standard Survey Method
