MEF2C-Related 5q14.3 Microdeletion Syndrome Detected by Array CGH: A Case Report
- Affiliations
-
- 1Department of Rehabilitation Medicine, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- 2Genetics Laboratory, Fertility Center of CHA Gangnam Medical Center, CHA University, Seoul, Korea. shshim@cha.ac.kr
- 3Department of Biomedical Science, College of Life Science, CHA University, Pocheon, Korea.
- KMID: 2165653
- DOI: http://doi.org/10.5535/arm.2015.39.3.482
Abstract
- Genetic screening is being widely applied to trace the origin of global developmental delay or intellectual disability. The 5q14.3 microdeletion has recently been uncovered as a clinical syndrome presenting with severe intellectual disability, limited walking ability, febrile convulsions, absence of speech, and minor brain malformations. MEF2C was suggested as a gene mainly responsible for the 5q14.3 microdeletion syndrome. We present the case of a 6-year-old girl, who is the first patient in Korea with de novo interstitial microdeletions involving 5q14.3, showing the typical clinical features of 5q14.3 microdeletion syndrome with a smaller size of chromosomal involvement compared to the previous reports. The microdeletion was not detected by subtelomeric multiplex ligation-dependent probe amplification, but by array comparative genomic hybridization, which is advisable for the detection of a small-sized genetic abnormality.
MeSH Terms
Figure
-
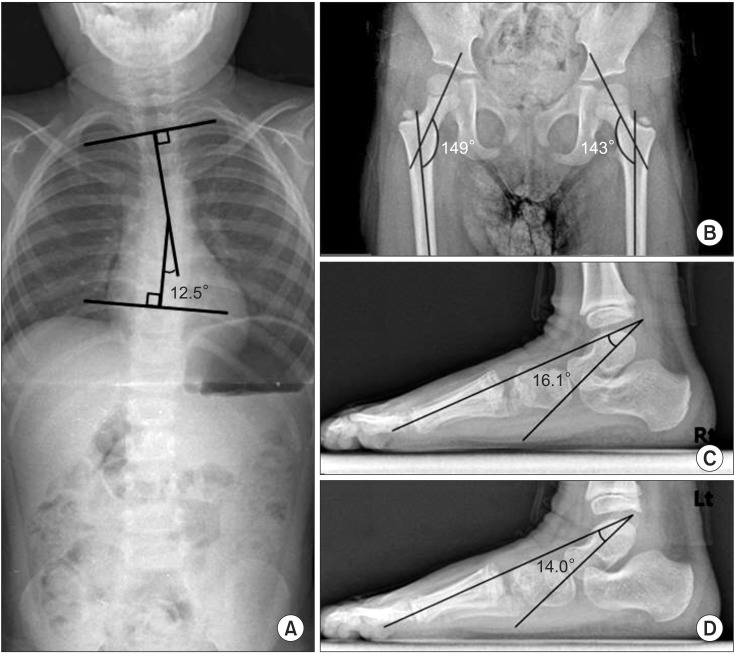
Fig. 1 Plain X-ray films of the patient showed mild thoracic scoliosis with Cobb's angle of 12.5° (A), left pelvic tilting, bilateral coxa valga with the angle between the axis of femur neck and shaft of 149° and 143°, respectively (B), and bilateral pes planus of talometatarsal angle of 16.1° (C) and 14.0° (D). The patient was unable to stand still with her ankles in a neutral position while taking the plain X-rays.
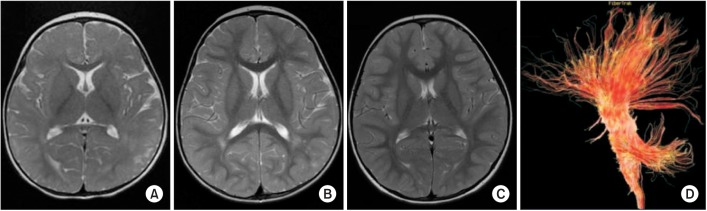
Fig. 2 Brain magnetic resonance imaging (MRI) of the patient showed delayed myelination at both 10 months (A) and 19 months (B), showing a prominent T2 high signal in the parietal deep white matter. A follow-up MRI at 48 months (C) had no focal abnormality. Diffusion tensor tractography showed normal microstructure (D).
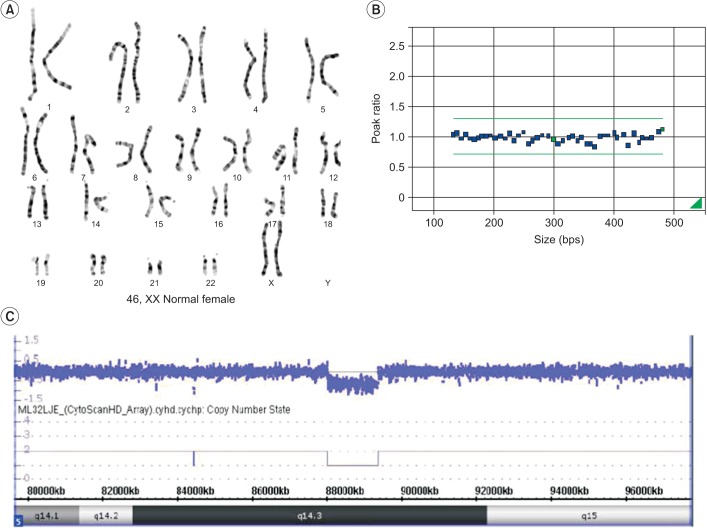
Fig. 3 Chromosome analysis of the proband (A) and multiplex ligation-dependent probe amplification analysis using a subtelomeric probe set (P070) (B) showed a normal female karyotype for our patient. However, the oligonucleotide array comparative genomic hybridization profile (C) showed a 1.33-Mb sized deletion in the 5q14.3 region.
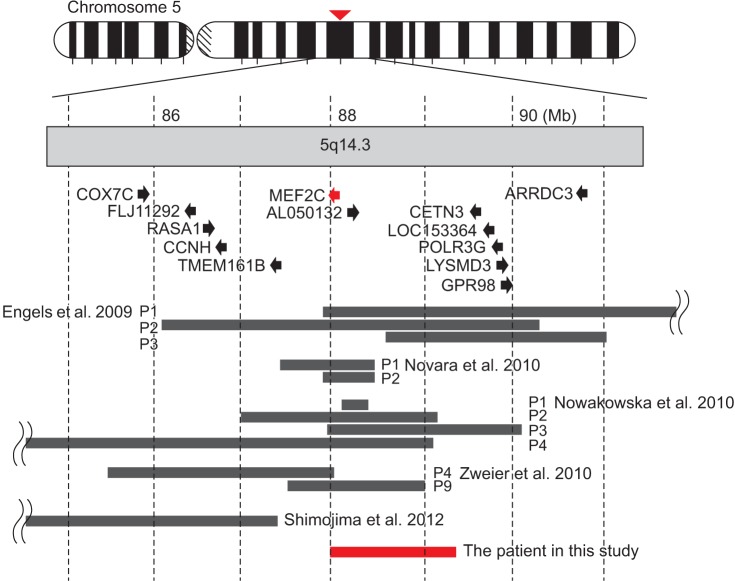
Fig. 4 Schematic representation of the deletions in chromosome 5q14.3 from all the previous reports (black bars) and our patient in this study (red bar). Black arrows represent the direction and the length of genes in this region. Modified from Shimojima et al. [6] with permission of John Wiley & Sons.
Reference
-
1. Hunter AG. Outcome of the routine assessment of patients with mental retardation in a genetics clinic. Am J Med Genet. 2000; 90:60–68. PMID: 10602119.
Article2. Szabo GP, Bessenyei B, Balogh E, Ujfalusi A, Szakszon K, Olah E. Detection of subtelomeric chromosomal rearrangements in idiopathic mental retardation. Orv Hetil. 2010; 151:1091–1098. PMID: 20558358.3. Engels H, Wohlleber E, Zink A, Hoyer J, Ludwig KU, Brockschmidt FF, et al. A novel microdeletion syndrome involving 5q14.3-q15: clinical and molecular cytogenetic characterization of three patients. Eur J Hum Genet. 2009; 17:1592–1599. PMID: 19471318.
Article4. Zweier M, Gregor A, Zweier C, Engels H, Sticht H, Wohlleber E, et al. Mutations in MEF2C from the 5q14.3q15 microdeletion syndrome region are a frequent cause of severe mental retardation and diminish MECP2 and CDKL5 expression. Hum Mutat. 2010; 31:722–733. PMID: 20513142.
Article5. Potthoff MJ, Olson EN. MEF2: a central regulator of diverse developmental programs. Development. 2007; 134:4131–4140. PMID: 17959722.
Article6. Shimojima K, Okumura A, Mori H, Abe S, Ikeno M, Shimizu T, et al. De novo microdeletion of 5q14.3 excluding MEF2C in a patient with infantile spasms, microcephaly, and agenesis of the corpus callosum. Am J Med Genet A. 2012; 158A:2272–2276. PMID: 22848023.7. Nowakowska BA, Obersztyn E, Szymanska K, Bekiesinska-Figatowska M, Xia Z, Ricks CB, et al. Severe mental retardation, seizures, and hypotonia due to deletions of MEF2C. Am J Med Genet B Neuropsychiatr Genet. 2010; 153B:1042–1051. PMID: 20333642.8. Novara F, Beri S, Giorda R, Ortibus E, Nageshappa S, Darra F, et al. Refining the phenotype associated with MEF2C haploinsufficiency. Clin Genet. 2010; 78:471–477. PMID: 20412115.9. Saitsu H, Igarashi N, Kato M, Okada I, Kosho T, Shimokawa O, et al. De novo 5q14.3 translocation 121.5-kb upstream of MEF2C in a patient with severe intellectual disability and early-onset epileptic encephalopathy. Am J Med Genet A. 2011; 155A:2879–2884. PMID: 21990267.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Overgrowth Syndrome with 9q22.3 Microdeletion Detected by Microarray Comparative Genomic Hybridization
- Identification of a Novel Deletion Region in 3q29 Microdeletion Syndrome by Oligonucleotide Array Comparative Genomic Hybridization
- Using Array-Based Comparative Genomic Hybridization to Diagnose Pallister-Killian Syndrome
- Array-based Comparative Genomic Hybridization and Its Application to Cancer Genomes and Human Genetics
- Analysis of Chromosomal Aberrations in Lung Cancer Cell Line, NCI-H1373
