Endoscopic Treatments of Endoscopic Retrograde Cholangiopancreatography-Related Duodenal Perforations
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea. thlee9@schmc.ac.kr
- 2Division of Gastroenterology, Department of Internal Medicine, Chungbuk National University College of Medicine, Cheongju, Korea.
Abstract
- Iatrogenic duodenal perforation associated with endoscopic retrograde cholangiopancreatography (ERCP) is a very uncommon complication that is often lethal. Perforations during ERCP are caused by endoscopic sphincterotomy, placement of biliary or duodenal stents, guidewire-related causes, and endoscopy itself. In particular, perforation of the medial or lateral duodenal wall usually requires prompt diagnosis and surgical management. Perforation can follow various clinical courses, and management depends on the cause of the perforation. Cases resulting from sphincterotomy or guidewire-induced perforation can be managed by conservative treatment and biliary diversion. The current standard treatment for perforation of the duodenal free wall is early surgical repair. However, several reports of primary endoscopic closure techniques using endoclip, endoloop, or newly developed endoscopic devices have recently been described, even for use in direct perforation of the duodenal wall.
MeSH Terms
Figure
-
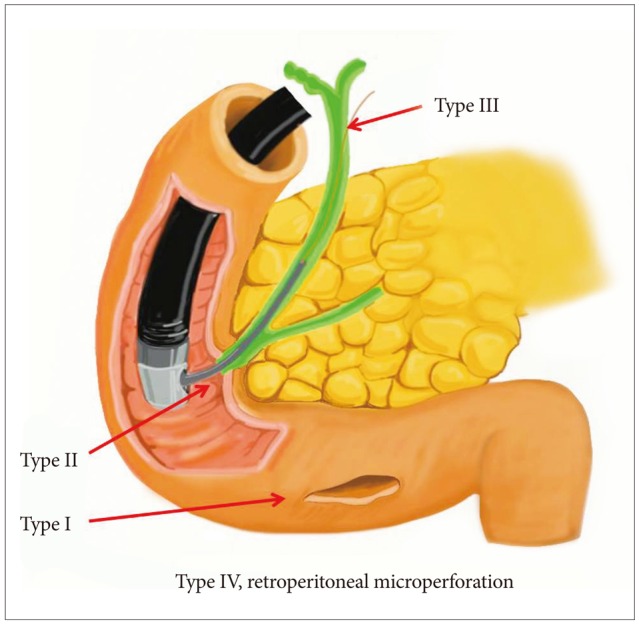
Fig. 1 Classical types of iatrogenic duodenal perforations: type I, endoscope-related lateral or medial duodenal wall perforation; type II, sphincterotomy-related periampullary perforations; type III, ductal or duodenal perforations due to endoscopic instruments such as a guidewire; type IV, retroperitoneal micoperforation caused by compressed air during endoscopy.
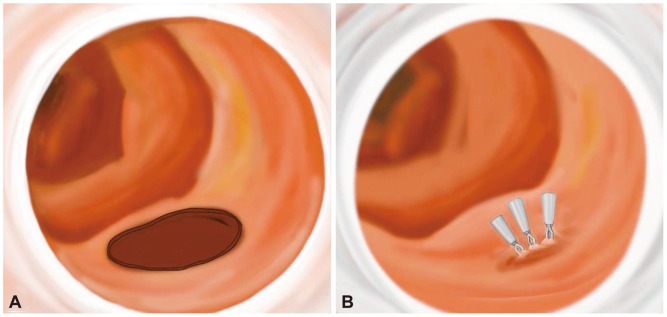
Fig. 2 Primary endoscopic closure using endoclips through a cap-fitted endoscopy. (A) Direct duodenoscope-induced duodenal wall perforation. (B) Simple endoscopic closure using multiple hemoclips via cap-fitted endoscopy.
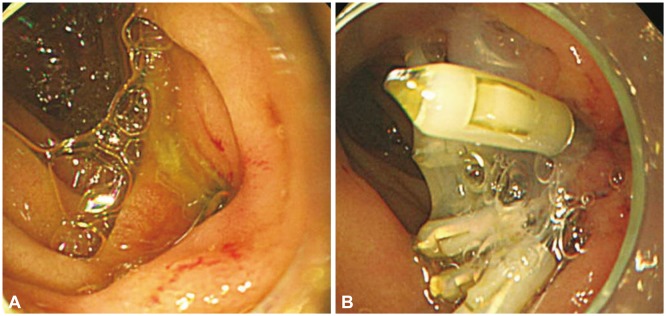
Fig. 3 Primary endoscopic closure using endoclips with glue injection in stent-induced duodenal wall perforation. (A) Cap-fitted endoscopy shows a circular perforated hole after removal of the stent. (B) The therapeutic attempt to generate primary closure using hemoclips and glue injection and spraying around the closed hole of the perforation.
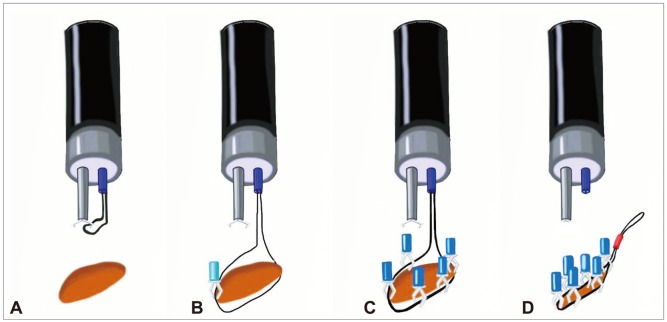
Fig. 4 Endoscopic closure of a large defect using an endoloop with multiple endoclips through 2-channel endoscopy. (A) Placement of endoscope and endoloop-containing catheter around the perforated area. (B) The tip of the endoloop is caught by the endoclip from the distal margin. (C) Multiple clips are attached with the endoloop to the perforated area. (D) The endoloop is tightened, thus closing the perforated area completely.

Fig. 5 Modified endoscopic closure using multiple endoloops with endoclips. (A) An endoloop was anchored with a clip to normal mucosa near the proximal resection margin. (B) The maneuver was repeated to anchor the same endoloop at the distal resection margin. (C) The endoloop was tightened slightly, resulting in approximation of the borders of the defect. (D) Another endoloop was required to bring the margins together. Additional clips can be placed to obtain complete wound closure if necessary.
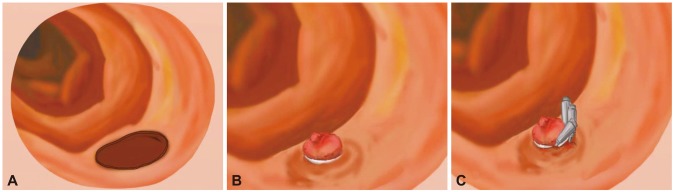
Fig. 6 Endoscopic band ligation (EBL) in an iatrogenic intestinal wall perforation. (A) Iatrogenic intestinal wall perforation after endoscopic mucosal resection or dissection. (B) Primary EBL was performed successfully in technical difficulty with endoclip closure. (C) Additional clips were applied around the band and surrounding mucosa.
Reference
-
1. Stapfer M, Selby RR, Stain SC, et al. Management of duodenal perforation after endoscopic retrograde cholangiopancreatography and sphin cterotomy. Ann Surg. 2000; 232:191–198. PMID: 10903596.2. Howard TJ, Tan T, Lehman GA, et al. Classification and management of perforations complicating endoscopic sphincterotomy. Surgery. 1999; 126:658–663. PMID: 10520912.
Article3. Enns R, Eloubeidi MA, Mergener K, et al. ERCP-related perforations: risk factors and management. Endoscopy. 2002; 34:293–298. PMID: 11932784.
Article4. Assalia A, Suissa A, Ilivitzki A, et al. Validity of clinical criteria in the management of endoscopic retrograde cholangiopancreatography related duodenal perforations. Arch Surg. 2007; 142:1059–1064. PMID: 18025334.5. Lee TH, Bang BW, Jeong JI, et al. Primary endoscopic approximation suture under cap-assisted endoscopy of an ERCP-induced duodenal perforation. World J Gastroenterol. 2010; 16:2305–2310. PMID: 20458771.
Article6. Vandervoort J, Soetikno RM, Tham TC, et al. Risk factors for complica tions after performance of ERCP. Gastrointest Endosc. 2002; 56:652–656. PMID: 12397271.7. Freeman ML. Complications of endoscopic biliary sphincterotomy: a review. Endoscopy. 1997; 29:288–297. PMID: 9255535.
Article8. Krims PE, Cotton PB. Papillotomy and functional disorders of the sphincter of Oddi. Endoscopy. 1988; 20(Suppl 1):203–206. PMID: 3049058.
Article9. Wu HM, Dixon E, May GR, Sutherland FR. Management of perforation after endoscopic retrograde cholangiopancreatography (ERCP): a population-based review. HPB. 2006; 8:393–399. PMID: 18333093.
Article10. Miller G, Yim D, Macari M, Harris M, Shamamian P. Retroperitoneal perforation of the duodenum from biliary stent erosion. Curr Surg. 2005; 62:512–515. PMID: 16125609.
Article11. Melita G, Currò G, Iapichino G, Princiotta S, Cucinotta E. Duodenal per foration secondary to biliary stent dislocation: a case report and review of the literature. Chir Ital. 2005; 57:385–388. PMID: 16231831.12. Sánchez-Tembleque MD, Naranjo Rodrìguez A, Ruiz Morales R, Hervás Molina AJ, Calero Ayala B, de Dios Vega JF. Duodenal perforation due to an endoscopic biliary prosthesis. Gastroenterol Hepatol. 2005; 28:225–227. PMID: 15811264.13. Kaneko T, Akamatsu T, Shimodaira K, et al. Nonsurgical treatment of duodenal perforation by endoscopic repair using a clipping device. Gastrointest Endosc. 1999; 50:410–413. PMID: 10462667.
Article14. Katsinelos P, Paroutoglou G, Papaziogas B, Beltsis A, Dimiropoulos S, Atmatzidis K. Treatment of a duodenal perforation secondary to an endoscopic sphincterotomy with clips. World J Gastroenterol. 2005; 11:6232–6234. PMID: 16273659.
Article15. Baron TH, Gostout CJ, Herman L. Hemoclip repair of a sphincterotomy-induced duodenal perforation. Gastrointest Endosc. 2000; 52:566–568. PMID: 11023583.
Article16. Baron TH, Wong Kee, Zielinski MD, Emura F, Fotoohi M, Kozarek RA. A comprehensive approach to the management of acute endoscopic perforations (with videos). Gastrointest Endosc. 2012; 76:838–859. PMID: 22831858.
Article17. Han JH, Lee TH, Jung Y, et al. Rescue endoscopic band ligation of iatrogenic gastric perforations following failed endoclip closure. World J Gastroenterol. 2013; 19:955–959. PMID: 23429885.
Article18. Kim KW, Lee TH, Park SH, et al. a primary repair with hemoclips and fibrin glue injection in biliary stent induced duodenal perforation. Korean J Gastrointest Endosc. 2011; 42:437–441.19. Marano BJ Jr, Bonanno CA. Metallic biliary endoprosthesis causing duodenal perforation and acute upper gastrointestinal bleeding. Gastrointest Endosc. 1994; 40(2 Pt 1):257–258. PMID: 8013842.
Article20. Mutignani M, Iacopini F, Dokas S, et al. Successful endoscopic closure of a lateral duodenal perforation at ERCP with fibrin glue. Gastrointest Endosc. 2006; 63:725–727. PMID: 16564890.
Article21. Seibert DG. Use of an endoscopic clipping device to repair a duodenal perforation. Endoscopy. 2003; 35:189. PMID: 12561015.
Article22. Sebastian S, Byrne AT, Torreggiani WC, Buckley M. Endoscopic closure of iatrogenic duodenal perforation during endoscopic ultrasound. Endoscopy. 2004; 36:245. PMID: 14986227.
Article23. Nakagawa Y, Nagai T, Soma W, et al. Endoscopic closure of a large ERCP-related lateral duodenal perforation by using endoloops and endoclips. Gastrointest Endosc. 2010; 72:216–217. PMID: 20304402.
Article24. Endo M, Inomata M, Terui T, et al. New endoscopic technique to close large mucosal defects after endoscopic mucosal resection in patients with gastric mucosal tumors. Dig Endosc. 2004; 16:372–375.
Article25. Matsuda T, Fujii T, Emura F, et al. Complete closure of a large defect after EMR of a lateral spreading colorectal tumor when using a two-channel colonoscope. Gastrointest Endosc. 2004; 60:836–838. PMID: 15557972.
Article26. Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy com plications and their management: an attempt at consensus. Gastrointest Endosc. 1991; 37:383–393. PMID: 2070995.27. Vezakis A, Fragulidis G, Nastos C, Yiallourou A, Polydorou A, Voros D. Closure of a persistent sphincterotomy-related duodenal perforation by placement of a covered self-expandable metallic biliary stent. World J Gastroenterol. 2011; 17:4539–4541. PMID: 22110286.
Article28. Park WY, Cho KB, Kim ES, Park KS. A case of ampullary perforation treated with a temporally covered metal stent. Clin Endosc. 2012; 45:177–180. PMID: 22866262.
Article29. Kwon CI, Song SH, Hahm KB, Ko KH. Unusual complications related to endoscopic retrograde cholangiopancreatography and its endoscopic treatment. Clin Endosc. 2013; 46:251–259. PMID: 23767036.
Article30. Shi Q, Chen T, Zhong YS, et al. Complete closure of large gastric defects after endoscopic full-thickness resection, using endoloop and metallic clip interrupted suture. Endoscopy. 2013; 45:329–334. PMID: 23468195.
Article31. Aliperti G. Complications related to diagnostic and therapeutic endoscopic retrograde cholangiopancreatography. Gastrointest Endosc Clin N Am. 1996; 6:379–407. PMID: 8673333.
Article32. Saranga Bharathi R, Rao P, Ghosh K. Iatrogenic duodenal perforations caused by endoscopic biliary stenting and stent migration: an update. Endoscopy. 2006; 38:1271–1274. PMID: 17163332.
Article33. Esterl RM Jr, St Laurent M, Bay MK, Speeg KV, Halff GA. Endoscopic biliary stent migration with small bowel perforation in a liver transplant recipient. J Clin Gastroenterol. 1997; 24:106–110. PMID: 9077729.34. Mastorakos DP, Milman PJ, Cohen R, Goldenberg SP. An unusual complication of a biliary stent-small bowel perforation of an incarcerated hernia sac. Am J Gastroenterol. 1998; 93:2533–2535. PMID: 9860420.
Article35. Coppola R, Masetti R, Riccioni ME, et al. Early retroduodenal perforation following endoscopic internal biliary drainage. Endoscopy. 1993; 25:255–256. PMID: 8519251.
Article36. Humar A, Barron PT, Sekar AS, Lum A. Pancreatitis and duodenal perforation as complications of an endoscopically placed biliary stent. Gastrointest Endosc. 1994; 40:365–366. PMID: 8056245.
Article37. Lee TH, Park SH, Son BS, et al. Four cases of guidewire induced periampullary perforation during endoscopic retrograde cholangiopancreatography. Korean J Gastrointest Endosc. 2011; 42:334–340.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Management of Endoscopic Retrograde Cholangiopancreatography-Related Duodenal Perforation
- Recent Advanced Endoscopic Management of Endoscopic Retrograde Cholangiopancreatography Related Duodenal Perforations
- Four Cases of Guidewire Induced Periampullary Perforation During Endoscopic Retrograde Cholangiopancreatography
- Two Cases of Successful ERCP during ERCP-Related Iatrogenic Duodenal Perforation
- Repair of an Endoscopic Retrograde Cholangiopancreatography-Related Large Duodenal Perforation Using Double Endoscopic Band Ligation and Endoclipping
